
PART I
INTRODUCTION
According to the coalition agreement of the Luxembourg Government 2023-2028 (p. 100):
“The cultivation of cannabis for personal use as it was legally regulated will be maintained. The Government will observe the position of the three neighbouring countries on the legalisation of cannabis.”
Although classed in the most restrictive schedules by the United Nations Single Convention on Narcotic Drugs of 1961,[1] at a time when little was known about its components and mechanisms of action, cannabis is still the most widely used illegal psychoactive drug in the world, including the European Union. Luxembourg is no exception. In fact, the latest estimates of the prevalence of cannabis use in the general population outline the following situation in Luxembourg:
Fig. 1a: National lifetime, 12-month and 30-day prevalence of cannabis use in different age groups (% valid) (EHIS, 2019)
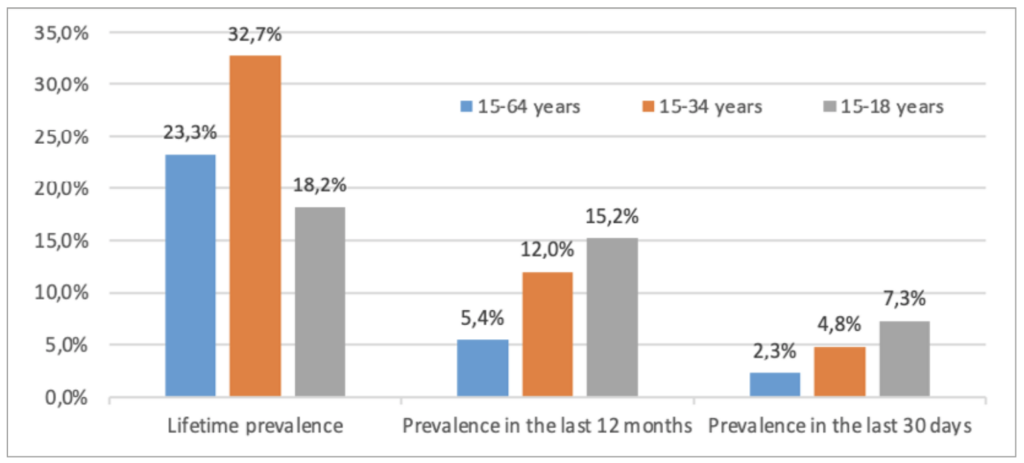
Source: European Health Interview Survey (EHIS), Luxembourg 2019, data processed by the Luxembourg National Focal Point of the EMCDDA
Lifetime prevalence of cannabis use (use at least once in a lifetime) is highest in young adults (15-34 years). Last-year and last-30-day prevalence in 15-18-year olds is, however, higher than that of older age groups and shows an upward trend (Figure 1a). The rate of prevalence, specifically over the last month is, however, one of the indicators of higher-risk use.
In contrast, the higher levels of lifetime prevalence of cannabis use compared to last 12-month or last-30-day prevalence indicate that most young people aged 15-34 who used cannabis did so experimentally or infrequently rather than regularly or continuously.
Although comparison of 2014 and 2019 data suggests an increase in cannabis use in all age groups (Figure 1b), these differences are not statistically significant:
- Experimental (lifetime) cannabis use in young adults (15-34 years) rose to 32.7% in 2019. Lifetime use in young people (15-18 years) increased from 16.6% in 2014 to 18.2% in 2019.
- Last-year cannabis use in the general population has increased since 2014. This increase was observed in young adults (15-34 years), and particularly in the youngest cohort (15-18 years).
- Last-month cannabis use shows an increase between 2014 and 2019, particularly in the youngest users (15-18 years), from 4.7% in 2014 to 7.3% in 2019.
Fig. 1b: Comparison of lifetime, last-year and last-month prevalence of cannabis use by different age groups (% valid) (EHIS, 2014, 2019)
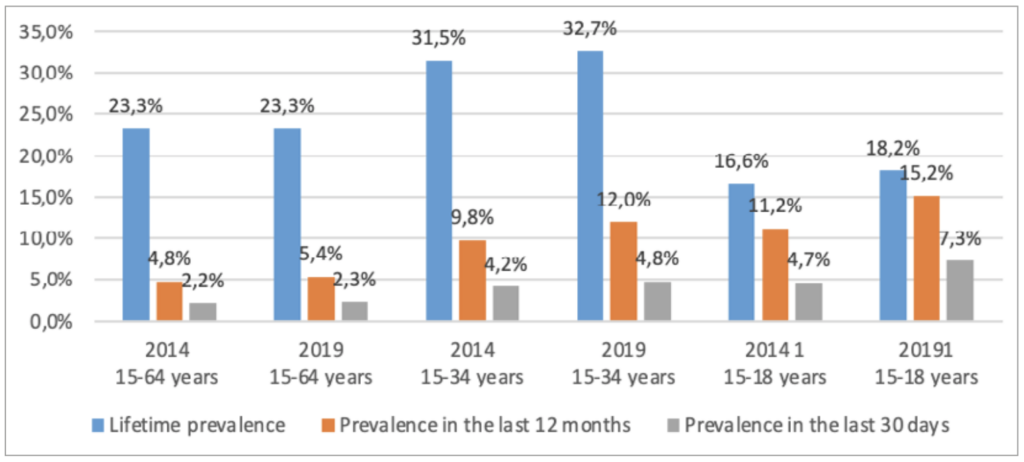 Source: European Health Interview Survey (EHIS), Luxembourg 2014, 2019, data processed by the Luxembourg National Focal Point of the EMCDDA
Source: European Health Interview Survey (EHIS), Luxembourg 2014, 2019, data processed by the Luxembourg National Focal Point of the EMCDDA
Gender differences are also worth noting. According to the latest estimates of the prevalence of cannabis use in the general population (EHIS 2014 and 2019), a higher proportion of men report having used cannabis than women(in their lifetime, as well as in the previous year and previous month). For example, in 2019, the prevalence of last-month cannabis use in men was more than double the prevalence of cannabis use in women (Figure 1c).
Fig. 1c: Prevalence of lifetime, last-year and last-month cannabis use in men and women: comparison of 2014 and 2019 data (EHIS, 2014, 2019)
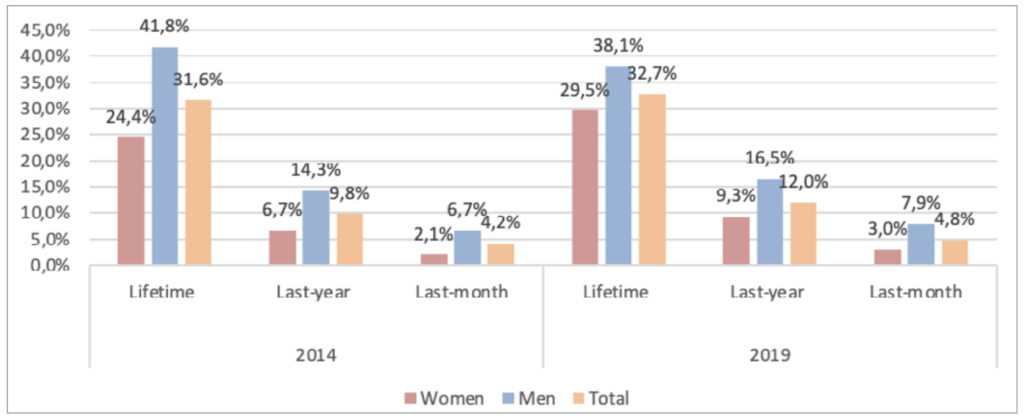 Source: European Health Interview Survey (EHIS), Luxembourg 2014, 2019, data processed by the Luxembourg National Focal Point of the EMCDDA
Source: European Health Interview Survey (EHIS), Luxembourg 2014, 2019, data processed by the Luxembourg National Focal Point of the EMCDDA
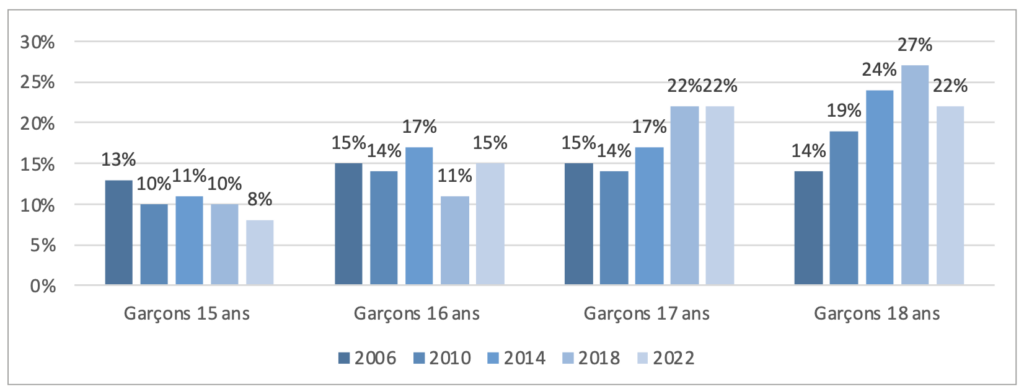
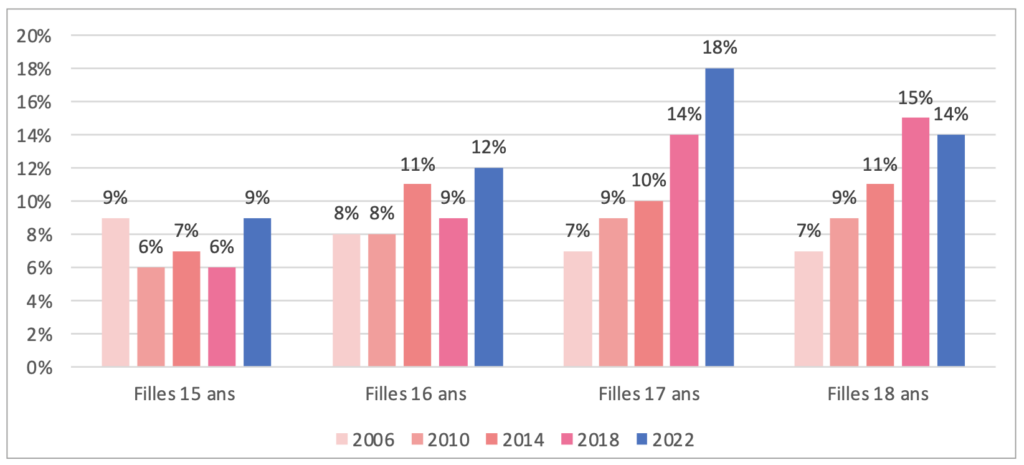
The results of the 2022 “Health Behaviour in School-Aged Children (HBSC)” study show that the lifetime prevalence of cannabis use in young people aged 15 to 18 years hardly changed at all between 2006 and 2022. Overall, the proportion of adolescents who report having used cannabis in their lifetime has remained stable. However, the proportion of adolescents who have used cannabis in the last 30 days has increased (see Figure 2a). Overall, in 2022, 13% of girls and 16% of boys aged 15 to 18 reported having used cannabis in the last 30 days (2018: 10% of girls and 16% of boys).
Fig. 2a: Lifetime and last-month prevalence of cannabis use in adolescents aged 15-18 years (% valid) (HBSC, 2006-2022)
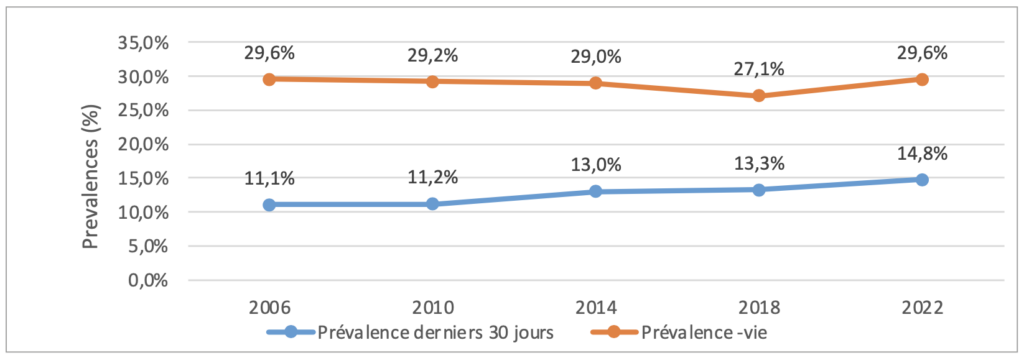 Source: Health Behaviour in School-aged Children (HBSC) Luxembourg, 2006-2022
Source: Health Behaviour in School-aged Children (HBSC) Luxembourg, 2006-2022
Analysis by age group reveals the following trends: in 2022, the percentage of girls and boys aged 17 to 18 who reported having used cannabis in the last 30 days increased compared to 2006. In 18-year-old girls, for example, this percentage doubled from 7% to 14% over the period. By contrast, in 15-year-old girls, the percentage remained stable at 9% (dropping from 13% to 8% for boys) (Figures 2b and 2c). Both indicators of cannabis use (lifetime and last 30-day prevalence) suggest that use has decreased in the youngest adolescents (15 years) and increased in older adolescents, especially in girls.
 Source: HBSC study, Luxembourg (University of Luxembourg, 2022)
Source: HBSC study, Luxembourg (University of Luxembourg, 2022)
 Source: HBSC study, Luxembourg (University of Luxembourg, 2022)
Source: HBSC study, Luxembourg (University of Luxembourg, 2022)
Even though cannabis is illegal, and despite the steps taken to prevent it being sold and used, cannabis is currently the most widely used psychoactive substance by young and not-so-young people.
In addition, the purity, i.e. the Δ-9-tetrahydrocannabinol (THC[2]) concentration in the various types of cannabis currently available on the black market, is steadily increasing. Since 2006, this concentration has doubled in the EU and Luxembourg. Cannabis seized in Luxembourg (resin and herbal, among others) in 2019 showed an average THC concentration of 18.4%; in 2021, an average THC concentration of 19.6% was found (Figure 3). When only cannabis products with a THC concentration of 1% or more are considered, the overall average purity of cannabis-based products reaches 20.8% in 2021. It is also worth noting that 22.4% of cannabis (mainly in the form of resin)seized in Luxembourg in 2021, 10% in 2020, 19% in 2019, and 16% in 2018, showed a THC concentration of more than 30%.[3],[4]
Also, an emergence of products with a high concentration of THC and a low content of cannabidiol (CBD), a molecule with no euphoric effect, was observed. These high THC concentrations represent an increased health and addiction risk. Unlike THC, the average CBD concentration in cannabis has been falling constantly since the early 2000s, leading to an imbalance between the THC and CBD concentrations in the drug.
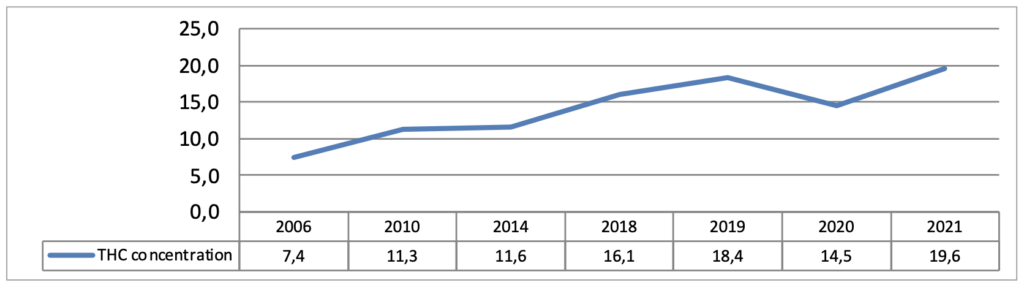 Source: Luxembourg National Health Laboratory, data processed by the Luxembourg National Focal Point of the EMCDDA, 2021
Source: Luxembourg National Health Laboratory, data processed by the Luxembourg National Focal Point of the EMCDDA, 2021
The highest THC levels in cannabis currently availably on the black market continue to break all-time records, in particular owing to increasingly refined extraction techniques and new varieties being cultivated. THC concentrations of 36 to 60% in various cannabis derivatives and extracts were recorded in 2019. In 2020, the maximum THC concentration observed in cannabis products was 72.7%, rising to an all-time high of 98.4% in 2021.[5]
In addition, the trend in THC concentrations, in relation to the price of cannabis products currently on the market, raises questions. The THC concentration of cannabis sold on the black market more than doubled between 2010 and 2020, while the price in Europe remained relatively stable over the same period (Figure 4).
Fig. 4: Average change in price and concentration of flowering tops in the EU (cannabis resin on the left, flowering tops on the right:
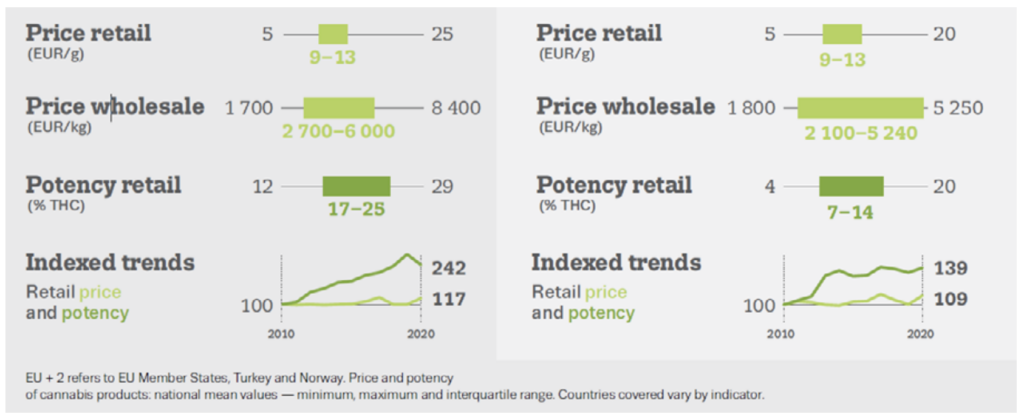 Source: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA, 2022)
Source: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA, 2022)
According to a sample of recreational drug users surveyed by the European Web Survey on Drugs (EWSD),[6]conducted in Luxembourg in 2018, cannabis prices averaged €14.5/g for resin and €16.7/g for herbal cannabis. The results of the latest EWSD conducted in Luxembourg in 2021 show that cannabis prices on the black market have fallen sharply to €9.0/g for resin and €10.1/g for herbal cannabis.[7]
In Luxembourg, the number of people in contact with specialist drug and addiction services due to their high-risk use of cannabis seems to have increased over the last few years, which may be linked, amongst other things, to the increased concentration of THC in cannabis products sold on the black market.[8]
In addition, most users are accustomed to smoking cannabis mixed with tobacco, a method of taking the drug that carries additional, and proven, health risks due to the combustion of various harmful substances and the risk of nicotine addiction.
To date, the quality of cannabis taken by the national population is driven by the black market. The cannabis sold on the black market is often adulterated and contains a wide variety of cutting agents (wax, soil, henna, paint, sand, talc, aromatic hydrocarbons, other herbs, pollen, microscopic glass beads, lead, etc.), many of which present an additional and significant health risk to users. In addition to these cutting agents, there are also risks of contamination with pesticides, microbes, heavy metals or even fungi.
Cannabis users are at the mercy of the criminal organisations that control the black market, where they also risk becoming victims of aggressive behaviour and of encountering other higher risk substances. Users break the law when they obtain cannabis which, in addition, is of uncertain quality and generates substantial revenue for organised crime, which has seen its power and growth margins increase considerably. This situation not only exposes users to increased health and safety risks, but also impacts on wider society. Illegal selling of cannabis in public places is increasingly perceived by the general public as alarming and disturbing.
A longitudinal analysis shows a further increase in the quantities of cannabis intended for the domestic market seized from 2014 onwards, with a new high in the amount of cannabis seized in 2019. In 2020 and 2021, the number of seizures (2021: 1,150 seizures; 2020: 1,142 seizures; 2019: 1,315 seizures) remained stable, although the quantities seized (2021: 53.3 kg; 2020: 102 kg; 2019: 371 kg) were down on 2019, but are still high and reflect the well-established presence of cannabis on the Luxembourg black market for drugs. Overall, seizures of cannabis-based products accounted for 74.1% of the total number of seizures in Luxembourg in 2021 (2020: 67.2%; 2019: 70.1%).[9] It is, however, worth noting that variations in drug seizures may also depend on the intensity of policing over a given period.
The present-day context of cannabis use is also based on the considerable change in the image of cannabis and its perception by the general public. Increased research into the composition and properties of cannabis and, in particular, the growing recognition of the use of cannabis for medical purposes, have contributed to this change of perception. This change has also taken place in Luxembourg, where the medical use of cannabis has been permitted under certain conditions since the entry into force of the Act of 20 July 2018[10] and its implementing regulations.
In addition, some jurisdictions have already legalised and regulated access to non-medicinal cannabis, including Canada, Uruguay and many US states, although practical implementation in these countries and states often differs. In addition to these countries and jurisdictions, many other countries are currently engaged in discussions and work on regulating access to non-medical cannabis, such as Germany, the Netherlands, the Czech Republic, Malta, Colombia, Costa Rica, Mexico, New Zealand, Jamaica, Israel and South Africa. In these countries, the search for alternative and sustainable models and approaches is based on the lessons learned from the inadequacy of some current legislative approaches to the sale and use of cannabis when compared to their intended purpose and on a desire to provide a regulatory framework for a widespread and growing phenomenon that is clearly resistant to law enforcement measures. In fact, approaches and regulations adopting prohibition, law enforcement and punitive responses as basic principles have not delivered the desired results in many countries.
The pilot project for legal access to cannabis for non-medical purposes is similar to regulations adopted to deal with the dangers of alcohol or tobacco use. In fact, it can be argued that it is the government’s responsibility to regulate and minimise the risks associated with products or substances that are taken by a significant proportion of the population and whose use is potentially high risk. The idea that the prohibition of alcohol and/or tobacco would be an appropriate, reasonable and effective solution to preventing the use and/or abuse of these psychoactive substances, some of which, like alcohol, are known to be more harmful than cannabis,[11] has never been seriously considered by European governments in recent decades. An exclusively punitive approach is, therefore, open to criticism.
In addition, the pilot project envisaged by Luxembourg is in line with the national approach generally taken in the field of drugs and addiction, which for two decades now has recognised the worth of harm- and risk-reduction measures in relation to drugs and addiction. The pilot project for legal access to cannabis for non-medical purposes is, therefore, just an extension of a public healthcare and public order rationale and a risk- and harm-reduction approach that has now been legitimised in lots of European countries and, in addition, is advocated by the European Union[12].
Existing global models for regulating access to cannabis for non-medical purposes differ insofar as they take into consideration national differences and characteristics in order to arrive at appropriate and effective solutions. Luxembourg will, therefore, have to adopt a national approach that takes into account its own cultural, social and economic parameters.
In view of the proposed regulation of cannabis for non-medical purposes announced by the Government of Luxembourg on 22 October 2021, in particular, as a first stage in a package of measures on the problem of drug-related crime, data allowing for a proper and nuanced assessment of the situation regarding cannabis and its use are required.
It is worth noting that this is an empirical approach, given that the national pilot project will be subject to scientific evaluation based on relevant impact indicators, which are key to adapting and developing the pilot project to meet requirements in the territory of Luxembourg. This scientific evaluation will be carried out in close collaboration with the EMCDDA and its National Focal Point, and with various public health research institutions. In addition, and as part of a more general evaluation, reports will be prepared describing the situation before the law comes into force and at regular periods thereafter. To this end, studies will be conducted in collaboration with research institutions and with the support of the EMCDDA, to assess specific indicators related to the implementation of the pilot project for legal access to cannabis for non-medical purposes.
A goal-oriented evaluation of the changes observed as a result of the future regulation presupposes that the relevant data have been collected before the law comes into force (baseline) and then at regular intervals during the rollout of the new measures.
To this end, a “Scientific Evaluation” working group was set up to compile a set of relevant indicators and the overall architecture of the evaluation exercise. In the first instance, national objectives were clearly defined in order to determine the relevant indicators.
[1] In the United Nations Single Convention on Narcotic Drugs of 1961, cannabis is listed in Schedules I and IV alongside substances like heroin, desomorphine, etc.
[2] European Monitoring Centre for Drugs and Drug Addiction (EMCDDA): The main psychoactive ingredient in all cannabis-based products is Δ9- tetrahydrocannabinol.
[3] Luxembourg National Health Laboratory. (2021). 2006-2021 data on the purity of illegal psychoactive substances processed by the EMCDDA Luxembourg Focal Point. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
[4] In 2019, 22.4% of samples had a THC concentration above 30%.
[5] Luxembourg National Health Laboratory (2021) 2021 data on the purity of illegal psychoactive substances processed by the EMCDDA Luxembourg Focal Point. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
[6] Trend data not available.
Berndt, N., & Seixas, R. (2019). Enquête Européen sur les Drogues au G.D. de Luxembourg 2018. EMCDDA Luxembourg Focal Point, Epidemiology and Statistics Department, Health Directorate: Luxembourg.
[7]Kugener, T., Berndt, N. & Seixas, R. (manuscript in preparation). Enquête Européen sur les Drogues au G.D. de Luxembourg 2021. Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health: Luxembourg.
[8] Berndt, N., Seixas, R., Origer, A. (2021). National Drug Report 2021 (Rapport RELIS) – The drug phenomenon in the Grand Duchy of Luxembourg: Trends and Developments, Epidemiology and Statistics Department, Directorate of Health: Luxembourg.
[9] Luxembourg Judicial Police Service – Drug Squad (2021) Data on drug seizures processed by the EMCDDA Luxembourg Focal Point. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
[10] Luxembourg Ministry of State – Central Legislative Service (2018) Act of 20 July 2018 amending the amended Act of 19 February 1973 on the sale of medicinal substances and the fight against drug addiction. Publication: 01/08/2018; Effective date: 05/08/2018. Luxembourg: Ministry of State – Central Legislative Service. Available at: http://data.legilux.public.lu/eli/etat/leg/loi/2018/07/20/a638/jo
[11] Nutt, D., King, L.A., Saulsbury, W., Blakemore, C. (2007). Development of a rational scale to assess the harm of drugs of potential misuse. The Lancet, 369(9566):1047-53. DOI: 10.1016/S0140-6736(07)60464-4.
[12] Council of the European Union (2003). Council Recommendation of 18 June 2003 (2003/488/EC) on the prevention and reduction of health-related harm associated with drug dependence, OJ 3.7.2003, L 165/31. Brussels: Official Journal of the European Union. Available at: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2003:165:0031:0033:EN:PDF
Clearly, the pilot project for legal access to cannabis for non-medical purposes should not aim to promote, or even to normalise or trivialise its use, but rather to make it possible to scientifically assess whether managing its use for non-medical purposes will reduce associated risks and harm, remembering that cannabis use has been going on for decades, despite its illegality.
The working group believes that the proposed pilot project can help to develop an evidence-based scientific foundation for decisions on possible future changes to the law. The evidence obtained from a scientific assessment (see II.3) should be methodologically sound, leading to scientifically valid knowledge as well as contributing to the objectivity of the debate and future orientations.
A scientific experiment (pilot project), limited in time and scope, is believed to be the most appropriate way to achieve the objectives sought, as described below.
An approach with public health at its core
The health of users of cannabis obtained on the black market is exposed to increased risk. As described above, in the course of the last 15 years, the THC content of cannabis and related products has significantly increased, while their CBD content has been significantly reduced; their price, meanwhile, has remained relatively stable (see Fig. 6). The quality of cannabis available on the black market is unpredictable (impurities, THC concentration, pesticides, adulterants, etc.) and there is a complete lack of any reliable way for users to determine, in particular, the THC and CBD content of products bought illegally.
Given that the potential harm associated with cannabis use is greater early on in life and/or with frequent use, the working group recommends that the government’s primary public health objectives should be as follows:
- To ensure product quality (THC and CBD content, absence of impurities and contamination, cutting agents, etc.) and product safety (e.g. plain packaging, warning labels), so that users know what they are taking and are able to make informed choices.
- To reduce high-risk use and addiction.
- To reduce the frequency and intensity of cannabis use, in particular cannabis with high THC and low CBD concentrations.
- To reduce the prevalence of high-risk methods of use (e.g. smoking cannabis with tobacco).
- To increase the age at which people start using cannabis.
- To protect young people by bolstering preventive measures and reducing cannabis use.
- To reduce the attractiveness and prevalence of synthetic cannabinoid use.
To use evidence-based information, education, health promotion and prevention strategies (universal, indicated, selective and environmental):
- To raise public awareness of the potential risks and damage to physical and mental health and to societylinked to cannabis, in particular, relating to regular high-risk use.
- To inform the public of the variability of cannabis quality, of the psychoactive effects of cannabis use and of the importance of concentrations, in particular, THC and CBD content.
- To bring about cannabis use that is more responsible, by providing information on the risks associated with the different frequencies/intensities of cannabis use.
- To promote methods of taking cannabis that are less damaging to health, particularly in view of the widespread habits in Luxembourg of smoking it with tobacco or of using it at the same time as drinking alcohol.
- To raise users’ awareness of the risks associated with using multiple psychoactive substances at once.
- To make users aware of their responsibilities and enhance their decision-making skills so that they can make informed choices, with a view to achieving a change in attitudes and behaviours towards less risky methods of taking cannabis, and of the fact that the lowest-risk type of behaviour in this area is abstinence. Raising awareness of the potential risks of the cannabis varieties used, as well as specific labelling of THC and CBD content and a colour-coded risk score, could help to achieve this objective.
- To increase the availability of and access to prevention programmes and risk-reduction services, in particular for socially disadvantaged groups and young people.
- To increase the availability of appointments and access to out- and in-patient treatment for the various target groups.
In addition to the above-mentioned public health objectives, other objectives include:
- To reduce the risks associated with the currently unavoidable exposure of users to the dangers associated with acquiring cannabis on black markets.
- To reduce social risks by helping to prevent users from entering the justice system (criminalisation, stigmatisation, etc.) and by keeping users away from the black market and criminal networks.
- To fight crime on the supply side, reducing the profit-generating activities of organised crime and helping to dry up an underground economy linked to drug trafficking, given that the revenue generated by the black market currently fuels the power of organised crime, increases its room for manoeuvre and aids its growth. These conditions, created by, among other things, the black market, can encourage the emergence and proliferation of societies and organisations in no-go areas that are detrimental to social cohesion and inclusion.
- To free up capacity and resources to reduce supply and use an approach less focused on punishment, thereby relieving police forces and the courts of the burden of prosecuting minor drug offences so that available resources can be focused on increasing the fight against organised crime.
- To closely monitor cannabis use at the national level to better understand patterns and trends of use in different population groups and to ensure the collection of longitudinal, comparable and nuanced data. These data will also make it possible to assess the impact of the pilot project for legal access and to make adjustments, as well as contributing, in the long term, to proactive investment in an integrated public health initiative that prioritises prevention and treatment. The data collected will also enable Luxembourg to contribute to international scientific literature on cannabis markets, cannabis use, public health implications and the potential consequences of legislative change.
- To develop pricing policies to discourage the use of cannabis with high THC content and increased health risks. The end price should, therefore, better reflect the potentially higher risks and harms of these cannabis products for users and for society.
1.4.1 For international and European law
As far as international law is concerned, the current international control and classification system for narcotic drugs was established by the United Nations Single Convention on Narcotic Drugs of 1961. This system currently comprises three conventions (to which Luxembourg is a party), namely:
- the United Nations Single Convention on Narcotic Drugs of 1961, as amended by the 1972 Protocol;
- the Convention on Psychotropic Substances of 1971;
- the United Nations Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances of 1988.
The protection of public health and well-being is at the heart of international and European drug legislation. Luxembourg has always pursued these same objectives and does not intend to deviate from this paradigm with this pilot project. Following a long-standing national policy of cracking down on cannabis use and promoting addiction prevention, and in view of the poor results achieved by the punitive approach, Luxembourg wishes to launch a pilot project that addresses the social phenomenon of large-scale cannabis use in the general population. International instruments give national legislators some leeway in determining the measures needed to implement obligations, and do not preclude trials for scientific purposes. This temporary and reversible scientific pilot project is, therefore, in line with the logic, and general spirit, of the international conventions. The pilot project’s precise relationship with international and European law will depend on the specific scope of the legal framework, its implementation and the legislative impact analysis.
It is worth noting that some regions of the world have seen a shift in opinion, with new approaches, on how to regulate access to cannabis. For this reason, with regard to international legislation, lines of communication will have to be kept open with other countries opting for a policy similar to that of Luxembourg, as well as with international organisations with expertise in this field. Within this context, the 2019 WHO recommendations on the reclassification of cannabis and related substances should also be taken into consideration.[1] At the same time, Luxembourg will have to keep dialogue open with the European Commission and neighbouring countries to inform them of the national impact of the pilot project. Further analysis is needed on how a pilot project on access to cannabis for non-medical purposes would fit with EU and international law, and on the development of a multi-dimensional communication strategy.
In any event, Luxembourg will maintain its commitment to the importance of the rule of international law, and in general, to multilateralism.
In this spirit, many bilateral and multilateral consultations and exchanges have taken place and will continue to be developed.
1.4.2 In terms of epidemiology and public health
Increased prevalence of cannabis use
It cannot be ruled out that legal access to cannabis will lead to temporary or sustained increases in cannabis use, or even tobacco use, for those who use smoke cannabis with tobacco. In line with the public health approach recommended, particular importance should, therefore, be attached to the measures that need to be taken to prevent a possible increase (whether temporary or persistent) in the prevalence and frequency of cannabis and tobacco use, especially in young people. Particular emphasis should, therefore, be placed on information, education and awareness-raising measures for the various target groups.
It is key to note that the still small number of studies on the effects of legalisation measures regulating access to non-medical cannabis provide mixed and inconclusive results.[2][3]Many factors are at play, and may be substantially influenced by higher rates of monitoring and testing. In addition, the importance of prevalence of use as an indicator of the impact, or even the merits, of drug policy is often overestimated, to the detriment of equally, or even more important indicators, such as high-risk use or the impact of such use on users’ mental health.
Even with robust longitudinal data it is, therefore, difficult to know what the drivers of change are and, in particular, to what extent any change in policy or legislation is material, causal or merely consequential.
In any event, these findings must be qualified insofar as the Luxembourg context differs from that of other jurisdictions. Some of these other jurisdictions, such as Canada, Uruguay, and some US states, have only recently started to evaluate the effects of legislation regulating access to cannabis for non-medical purposes. Most of these jurisdictions have only recently adopted legislation legalising access to cannabis for non-medical purposes. It would, therefore, be premature to draw definitive conclusions on their impact on public health indicators.
Some of these jurisdictions, and in particular the US states concerned, have adopted a legalisation system which gives market dynamics a significant role to play in regulation and, consequently, makes room for private entrepreneurship. The first evaluation data made available in certain countries or jurisdictions cannot, therefore, automatically be transposed to Luxembourg, which has specific forms of use and will adopt its own method of regulation.
In general, international studies show that it is necessary to go beyond analysis of the prevalence indicator alone in order to fully understand the impact that a change in access to cannabis, or any other psychoactive substance, may have (e.g. number of medical emergency episodes, hospital admissions and treatment requests related to cannabis use). In addition, comparisons of the situation before and after the pilot project are required. Consequently, a research proposal, including an analysis of the initial reference situation (baseline), is required.
Age criterion
The question of the minimum age of legal access to cannabis presents the legislator with a dilemma that can only be resolved through compromise. There is no single, perfect answer to this question. In fact, setting the age limit for legal access at 18 does not fully take into account the results of scientific research on brain development and the potential associated damage. On the other hand, setting the minimum age at 21 or 25 means depriving the segment of the general population in which cannabis use is most widespread (including minors), of legal, quality-controlled cannabis, and exposing it to the supply and risks of the residual black market. In addition, clashing with the criminal justice system can have consequences for the educational, employment and social inclusion chances of many users. Setting the age of legal access to cannabis at 21 or 25 could also result in alcohol being perceived as less harmful by young and old alike, whereas most analyses suggest the opposite is the case.
In addition, in our societies, the age of majority represents individual responsibility[3]. It may, therefore, seem questionable, or even contradictory, to hold 18-year-olds responsible for every aspect of their lives apart from their choice to use cannabis.
Simply introducing a legal age limit of 18 years for legal access to cannabis for non-medical purposes will not simultaneously remove the attraction of this substance and its effects on young people and minors, especially as many young people already use cannabis before the age of 18.
It could be argued that setting the age criterion for acquiring cannabis for non-medical purposes at 18 could leave young people under the age of 18 who are looking for cannabis with no choice but to seek it on the black market. This may even encourage drug dealers to adopt more targeted and aggressive sales strategies towards people under the age of 18 in order to compensate for the loss of revenue caused by the introduction of legal access to cannabis for non-medical purposes for adults aged 18 and over. Canada has tried to address this situation by decriminalising the possession of up to five grams of cannabis for young people under the age of 18, where it is for personal use and is not linked to cannabis trafficking.
If the risk of a possible increase in traffickers using aggressive sales techniques targeted at minors, is combined with the possibility that some adults may obtain cannabis legally and sell it to minors, the risk of increased exposure of minors to cannabis cannot be eliminated, which in turn may lead to an increase in use, and frequency of use, in a population considered particularly vulnerable from a psychological and physical point of view.
In fact, the use of cannabis with a high THC content is more risky the earlier in life a person takes it and it can negatively affect brain development in children, adolescents and young adults. It is currently accepted that the main developments in brain maturity and connectivity are complete around the age of 25. The potential harm caused by regular use of cannabis with high THC content is considered to be at its greatest before this age.
What’s more, cannabis use in adults is not without risk. It can lead to desocialisation, or even trigger psychotic decompensation in predisposed individuals (family history of psychotic disorders) and depending on the method of use (e.g. early use of cannabis, use of cannabis high in THC and low in CBD). It is worth noting that these risks increase with the THC and CBD content of cannabis, which has been steadily rising and falling respectively over the last decade.
In addition, perception of the risks associated with cannabis use may diminish and, as a result, cannabis use may be normalised or trivialised. It therefore seems useful to explain to the public that access to cannabis is not regulated in the pilot project because it is risk-free, but because the negative side effects of a punitive response to cannabis use are greater and because it is reasonable and necessary to consider whether other approaches might not be better suited to reducing health and safety risks and associated illegal activities.
The important thing about setting the legal age of access at 18 – which, let us remember is, in the case in point, nothing more than one tenable compromise – is not to punish offending minors indiscriminately, but to take advantage of this opportunity to discuss with the young people concerned their use, or even high-risk use, and the context of this use, and to make it a fully fledged prevention and risk-reduction tool.
In any event, the young people in question should be involved in early interventions in groups, or on an individual basis, to make them aware of the risks associated with their use of cannabis or other drugs.
Offers of prevention, (early) counselling and care for young people are available nationwide. These have been developed in close cooperation with the Ministry of Health, the Public Prosecutor’s Office and specialist services and are designed specifically for interaction with young people, particularly where an offence has been committed, allowing them to access a structured programme to help them come to terms with the current situation and to develop their skills and evaluation capabilities.
In addition to these measures, it is essential to develop and implement a comprehensive information, education, prevention and communication strategy specifically targeting young people (see chapter on prevention).
Road safety
Legal access to cannabis may have implications for road safety, although driving under the influence of cannabis is already an observable phenomenon today.
It is important for any change in approach and any legislative change in the area of legal access to cannabis to be accompanied by a coherent information, prevention and care strategy. The aim is to increase drivers’ awareness that driving under the influence of cannabis involves risks both for them and others.
In accordance with the law of 14 February 1955, on traffic regulation on all public highways, any driver of a vehicle or animal, as well as any pedestrian involved in an accident, whose body contains a serum THC level of 1ng/ml or more, shall be punished by imprisonment of between eight days and three years and a fine of between €500 and €10,000, or one of these penalties only.
Public health authorities will be responsible for supporting policing activities through education and awareness-raising of the dangers of driving after using cannabis.
Likewise, a simultaneous stepping-up of the law enforcement response to any activities outside the framework of the pilot project would seem appropriate. In addition, a research and monitoring system must be set up to validly measure the impact of the measures adopted in order to be able to progressively assess their feasibility and the possible need to extend them, or even to reconsider or develop them at a later date.
Currently, the Highway Code provides for a critical threshold of 1 ng/ml of THC in the bloodstream.[4]
It is recommended that expert advice be sought during the legislative process. This is to ensure that the measures in place are based on up-to-date, valid and robust scientific evidence that reliably detects whether the driver is fit to drive a vehicle or whether the driver’s faculties are impaired.
Safety at work/high-risk jobs:
Collective labour agreements, internal company regulations, etc. deal in various ways with being under the influence (of alcohol or other psychoactive substances) in the workplace. It is necessary to check whether cannabis use is covered by these provisions, bearing in mind that there is currently no simple method that can be used by non-experts to detect, at first sight, and without additional means of detection, someone who is under the influence of cannabis, unlike someone who is under the influence of alcohol (breath, slurred speech, etc.).
It is also recommended that expert advice be sought during the legislative process.
1.4.3 Financial and banking industry
The pilot project for legal access to cannabis for non-medical purposes could have an impact on the financial sector, in particular, due to European and international regulations in force (especially to combat money laundering), as well as the rules imposed by the United States. The Patriot Act prohibits US companies from having contact with foreign companies involved in, among other things, the trafficking of controlled substances, such as cannabis. In Uruguay, for example, banks have stopped all transactions connected with the sale of cannabis, even though sales are managed by state-run pharmacies, for fear of no longer being able to carry out transactions with the United States.
At this stage, the same difficulty does not appear to have been experienced on the Canadian side. Banks are, however, reportedly still very cautious and try to keep any cannabis-related transactions strictly separate from their US transactions. It is, therefore, worth examining this point in greater depth in order to determine the possible impact of the pilot project for legal access to cannabis for non-medical purposes on the financial and banking sector in Luxembourg.
With the pilot project in question, accepting customers operating in the cannabis-related production and/or marketing sectors, even if these activities have been legalised, is a matter for the banks’ own commercial policy. Those concerned cannot, therefore, be guaranteed an account.
As for the implications for compliance with international anti-money laundering rules, this point remains to be explored in greater depth as the models under consideration are put into practice.
In any event, all operators in the future regulated cannabis sector will be bound by a set of existing anti-money laundering rules. These include the obligation to conduct an assessment of the specific money laundering risks associated with the sector (e.g. cash, fraud, unlicensed traders and producers, etc.), taking into account the variables of the national economy and its different sectors, to determine the degree of risk that the sector(s) may pose, or to understand how these money laundering risks may affect the national or even supranational economy.
Where risks are identified, it is then the responsibility of the operators concerned to adapt their behaviour accordingly and to mitigate the risks involved by taking appropriate measures to limit these risks. An appropriate measure in this context would be to restrict, if not completely prohibit, the use of cash for all regulated cannabis-related transactions.
Apart from this specific risk assessment, operators in the cannabis field must also comply with a set of rules that apply to all professionals, such as customer due diligence, a procedure for establishing business relationships (professionals must avoid any business relationship with customers who do not wish to be transparent), the obligation to keep documents (for at least 5 years), to monitor vigilance, to report suspicions to the Financial Intelligence Unit (FIU), to have adequate internal organisation and to put in place written internal control and communication procedures, to proactively cooperate with the competent supervisory authorities, to appoint an internal manager and to provide adequate training to its employees.
Existing administrative and criminal penalties will also apply to those involved in the regulated cannabis sector.
1.4.4 Cannabis products with <0.3% THC
In recent years, many EU Member States, including Luxembourg, have seen the emergence of shops selling flowering tops, and other products extracted from cannabis plants, with a THC content of less than 0.3%.
In the context of, and in advance of, the recommended national pilot project, this aspect should also be managed to ensure the compatibility of these cannabis products with the approach described in the national pilot project for legal access to cannabis for non-medical purposes.
As a result, a dedicated interministerial working group has been set up to determine to what extent adjustments to the legal framework would be necessary.
1.4.5 Industrial hemp sector
The pilot project for legal access to cannabis for non-medical purposes could present new opportunities for industrial hemp cultivation in Luxembourg.
Hemp is one of the oldest plant species cultivated by humans. It was grown as far back as 4000 BC. This plant has also been grown in our region for thousands of years, not only for the production of cloth and rope (fibres), oil for food and other uses (seeds), but also for use as a natural medicine (flowers). In 1865, for example, industrial hemp cultivation in Luxembourg extended to some 700 hectares and was by far the most important oilseed and industrial crop in our country at that time.
As a result of developments in organic and pharmaceutical chemistry at the beginning of the 20th century, the products of hemp cultivation, such as fibres and flowers, had to compete with synthetic products, which led to the decline of industrial hemp cultivation in Europe and particularly in Luxembourg. After the First World War, the decline in industrial hemp accelerated dramatically until the plant, with its many advantages and potential uses, disappeared from Luxembourg completely.
The cultivation of industrial hemp only reappeared in our country about 25 years ago, following an initiative launched by several farmers who were looking for alternative crops to diversify their production and income. As a result, a network of several producers, involving cooperatives and private companies, based on the cultivation of industrial hemp with a low THC content (< 0.3%) and on the food value of the seeds and flowers, has since been successfully established. In addition, alongside this network with its very varied product range, the Chamber of Agriculture, in partnership with the FIL (Fördergemeinschaft Integrierte Landbewirtschaftung FIL Asbl) as part of the EFFO (Effiziente Fruchtfolgen) project, as well as the Agriculture Technical Services Administration (ASTA), set up industrial hemp trials on several experimental sites to study certain aspects of this crop with a view to helping to relaunch this ancestral plant, which has many advantages, both for the circular economy and for environmental protection, as well as for farmers and users.
In fact, this government’s coalition agreement explicitly provides for the development of industrial hemp in protected areas: “New crops, such as flax and hemp, present opportunities in a number of economic sectors as well as offering real added value for the environment. These crops will, in particular, be encouraged in protected areas”.
As a result, industrial hemp, which had been forgotten for more than a century, could once again have a major role to play in agriculture in Luxembourg and beyond because, as far as the Greater Region is concerned, intensive efforts are being undertaken to promote hemp fibre, also opening up opportunities for cooperation and outlets for Luxembourg producers.
Product varieties
Industrial hemp can be the basis for a wide range of products such as oil (food for human consumption, animal feed), fibre (textiles, insulation/construction, pellets/heating), hemp seed cake (solid residues obtained after extracting the oil from hemp seeds and intended for animal feed), flowers and flower extracts rich in CBD, (food for human consumption and animal feed). As a result, industrial hemp has the potential to become a key element of the bioeconomy and the circular economy, provided that intelligent and full use is made of the very many possibilities it offers i.e. stalks for producing fibres and hemp shives (the woody part of the hemp obtained and separated after scutching the fibre) as by-products, seeds for oil and hemp seed cake produced as by-products and flowers, and flower extracts (especially those rich in CBD) with numerous potential outlets.
This cascade use of industrial hemp, which is in line with how this plant was used traditionally for thousands of years, is not only sustainable and resource-efficient, but also recognises the fact that only full use of hemp, and all its by-products, will ultimately ensure the profitability of the industrial hemp sector.
Currently, more than 60 varieties of industrial hemp (with a low THC content < 0.3%) are already registered in the European Union (EU) Common Catalogue of Varieties of Industrial Plant Species (EU) and so are authorised for cultivation in the EU.[5] It is worth noting that outdoor open-field cultivation and the resulting flowers are not suitable for use in the cannabis products provided for within the context of the pilot project for legal access to cannabis for non-medical purposes.
Potential for the agricultural sector
Agriculture in Luxembourg, as elsewhere in Europe, is lacking in plant protein production and faces enormous challenges in protein autonomy. The use of hemp seed cake, which is very rich in protein, could help reduce national dependence on imported products. CO2 sequestration, as a result of the use of hemp fibres and shives, significantly increases the ecological balance of industrial hemp and is another opportunity for agriculture to join in the effort to mitigate greenhouse gases. The benefits of hemp in protecting soil and water are well known. Hemp could, therefore, become a crucial link in the crop-rotation chain.
Hemp only requires moderate nitrogen fertilisation and the 600-650 litre watering requirements are generally covered by the usual rainfall in Luxembourg. The deep roots of industrial hemp mean that the crop continues to grow when many other crops are already under considerable water stress. These deep roots have additional advantages in that they improve the biological activity of the soil and protect against soil erosion. The plant can also be grown on almost any type of soil in the country.
As a result of strong early growth, weeds barely invade the hemp, so fields are naturally weed-free during, and after, the cultivation of industrial hemp. Consequently, herbicide applications are very much reduced, or non-existent, for two years in a row. An industrial hemp harvest means that winter wheat can be grown under ideal conditions on weed-free plots as the next crop in the rotation.
Since the cultivation of hemp, for which neither weeds nor pests are a major problem, requires almost no use of plant protection products, it could partly replace rapeseed, another oilseed crop, the cultivation of which is declining, not least because of the great difficulties involved in protecting it from weeds and pests.
Better still, the incorporation of industrial hemp, which has no links to other plant species grown in Luxembourg, such as wheat, rape, barley, maize, etc., into existing agricultural rotations, will also have a positive effect on the health status of the follow-on crops, as hemp does not transmit harmful organisms to these crops and, by smothering weeds, leaves the fields weed-free for the follow-on crop. The cultivation of industrial hemp can, therefore, reduce the use of plant protection products throughout the entire crop rotation. As a result, industrial hemp also works well for crop rotation in organic farming.
Ultimately, the cultivation of industrial hemp not only expands the range of agricultural rotations which benefits the environment, in particular, by conserving water resources, but also increases indigenous protein production for animal feed, as well as offering farmers the chance to diversify and increase their income, provided that the industrial hemp is used in its entirety.
Up- and downstream potential for the sector
Alongside the primary agricultural sector, the development of industrial hemp cultivation could also have a positive impact on related up- and downstream sectors (seed production and certification, oil production, storage and production of concentrated animal feed, agricultural machinery, variety trials, research and development, small-scale production of industrial hemp products, renewable energy, heating fuels, etc.).
Potential for other sectors
In addition to the societal gain associated with direct sustainability benefits (soil, water, CO2 sequestration, etc.), the production of a range of fibre-based products for construction and insulation will have a positive effect on our carbon and ecological footprint across the nation. There is enormous potential in the use and extraction of industrial hemp flowers which could provide new sources of income for farms and specialist companies. In this regard, it would be advantageous to harmonise EU legislation on the commercialisation and use of industrial hemp flowers and flower extracts. The use of field-grown flowers offers the added benefit of not requiring the high energy input associated with indoor growing systems (intensive artificial lighting, heating) normally recommended for growing cannabis for medical and non-medical purposes.
[1] Upon examining a series of WHO recommendations on cannabis and its derivatives, the UN Commission on Narcotic Drugs decided to remove cannabis from Schedule IV of the United Nations Single Convention on Narcotic Drugs of 1961, where it was listed alongside other substances, including heroin, that were considered to have no significant therapeutic benefit.
[2] Cerdá, M., Wall, M., Feng, T., Keyes, K. M., Sarvet, A., Schulenberg, J., O’Malley, P. M., Pacula, R.L., et al. (2017). Association of state recreational marijuana laws with adolescent marijuana use. JAMA Pediatr, 171(2):142-9. DOI:10.1001/jamapediatrics.2016.3624
[3]Anderson, M., Hansen, B., Rees, D., Sabia, J. J. (2019). Association of Marijuana Laws with Teen Marijuana Use. JAMA Pediatr., 173(9):879-881. DOI:10.1001/jamapediatrics.2019.1720
[4] Ministry of Sustainable Development and Infrastructure (2016) Highway Code, General Plan, Article 12, paragraph four. Luxembourg: Ministry of Sustainable Development and Infrastructure. Available at: http://data.legilux.public.lu/file/eli-etat-leg-code-route-20161028-fr-pdf.pdf
[5] European Commission (2019) European Plant Variety Database. Available at: http://ec.europa.eu/food/plant/plant_propagation_material/plant_variety_catalogues_databases/search/public/index.cfm?event=SearchVariety&ctl_type=A&species_id=240&variety_name=&listed_in=0&show_current=on&show_deleted
PART II
LUXEMBOURG MODEL FOR THE PILOT PROJECT FOR LEGAL ACCESS TO CANNABIS FOR NON-MEDICAL PURPOSES
It is proposed that access to cannabis for non-medical purposes should be regulated by a rigorous and robust pilot project tailored to meet the Luxembourg’s specific needs. This fixed-term pilot project must be able to meet the challenges of the approach and achieve the objectives sought.
It should be noted that the pilot project for legal access to cannabis by the state differs from simple liberalisation, an approach where the regulation of supply and demand is supposed to be ensured by market forces and dynamics, with the state contenting itself simply with supervising market access, reducing informational asymmetries and defining the rules of “healthy” competition.
In terms of strategy for the creation and rollout of the pilot project for legal access to cannabis for non-medical purposes, the policy approach is to proceed in stages and to develop a specific approach to cannabis for non-medical purposes.
The first stage, bill No. 8033 amending the amended Act of 19 February 1973 on the sale of medicinal substances and the fight against drug addiction, was introduced on 22 June 2022. The legislative process is currently in progress.
With its risk reduction and crime prevention approach, the bill has a dual objective:
On the one hand, any person of legal age will be allowed to grow up to four cannabis plants, at home, per household, for personal use, exclusively from seed. It is worth noting that plants must be kept out of public view. Personal use in private will be allowed. If the place of cultivation is non-compliant or if the number of plants grown at home is exceeded, criminal penalties will apply.
On the other hand, there are plans to abolish criminal penalties for small quantities of cannabis (< 3 grams) in public. Less complex and swifter criminal proceedings will be introduced for adults in public possession of, or transporting and acquiring, no more than 3 grams of cannabis, or its derivatives (including mixed products). The bill reduces the range of fines to between €25 and €500 with the option for the Grand Ducal Police to issue a warning with a €145 fine. Use in public is still banned.
It is worth noting that this legalisation of self-cultivation and private use is a first step, pending finalisation of the overall concept to counteract the black market and regulate the illegal trade in cannabis. As appropriate, this first step will need to be reviewed and adapted, depending on the final system selected.
When drafting the bill implementing this concept note, the system introduced by bill No. 8033 will, therefore, be reassessed to ensure consistency between the two systems, particularly with regard to the issue of possession of cannabis in public.
To ensure the quality of cannabis and prevent the emergence of an unregulated parallel market for products of uncertain quality, regulations on the packaging and physical sale of cannabis seeds with a future THC content of more than 0.3% for private and personal use, will be put in place.[2]
[1] Bill No. 8033: https://www.chd.lu/fr/dossier/8033
[2] Draft grand-ducal regulation amending the amended grand-ducal regulation of 26 March 1974 setting out a list of narcotics.
At a later stage, the transition to legal access to cannabis for non-medical purposes will be ensured [1] and the following minimum criteria and conditions will have to be met:
- Be domiciled in Luxembourg: Actual residence in the Grand-Duchy of Luxembourg . This provision is intended to prevent “cannabis tourism”, to limit the potential disturbance caused by an increased influx of customers from all sides, and to increase acceptance, or even reduce fear, resistance and criticism from neighbouring countries[2];
- Age criterion: Minimum legal age, i.e. 18 years of age;
[1] As stated in the 2018 coalition agreement described in chapter I.1.
[2] In line with the decision of the European Union Court of Justice ruling on the compliance with EU law of a decision of the Mayor of Maastricht prohibiting coffee-shop owners from admitting to their establishments persons who are not actually resident in the Netherlands (Josemans, Case C-137/09).
For use in private only: The ban on taking cannabis and cannabis-derived products will apply to premises open to and/or serving the public, and to any places in which the ban on smoking (tobacco and e-cigarettes) applies. This measured is intended to limit public nuisances; prevent the passive inhalation of harmful, potentially psychoactive smoke by non-users; and to counter the spread and normalisation of cannabis use, and even the perception that it is less risky, among young and not-so-young people. The same rules must also apply to all other cannabis-based products smoked or vaped, in particular those with a THC content of less than 0.3%.
Maximum monthly and daily quantities: Given the domestic context, it is recommended that the monthly threshold should not exceed 30 grams of dried cannabis per customer. In addition, dispensaries will have to ensure, by means of a computer system common to all outlets, that the maximum quantity of 5 grams per day, per purchase and per customer, is not exceeded. These quantities purchased must be exclusively for personal use.
In order to make it easier to detect violations of the pilot project and ultimately ensure that it can be applied on a permanent basis, the working group believes that a distinction should be made between cannabis of legal, and illegal, origin. Relevant biomarker methods will have to be identified in order to determine, if necessary, the origin of the cannabis, bearing in mind the need for safety for the end-user and the importance of the price of legally available products remaining competitive with those for sale on the black market.
All relevant policies relating to smoking or drinking alcohol in the workplace should be adapted to incorporate the consumption of cannabis for non-medical purposes. In addition, a zero-tolerance rule should be applied to certain professions when carrying out their professional activity, such as pilots, police officers, surgeons, prison staff, professional drivers etc.
The working group recommends that the pilot project be accompanied by a scientific evaluation consisting of a pre- and post-implementation analysis based on validated scientific indicators. This scientific evaluation will be carried out in close collaboration with the EMCDDA and its National Focal Point, and with various public health research institutions. In addition, and as part of a general evaluation, these research institutions, with the support of the Luxembourg National Focal Point of the EMCDDA, will publish a final report on the first seven years after legal access to cannabis for non-medical purposes was introduced. Within this context, it is recommended that the scientific evaluation should also be supported by an independent and neutral committee of experts from different disciplines. The final research evaluation report should, therefore, include the conclusions of the evaluation exercise and, where appropriate, recommendations to be made to the government. It remains to be seen how long the committee will have to complete its evaluation and submit its report to the government before the scheduled end of the pilot project
After receiving the final evaluation report, the government will have a set amount of time, which is still to be determined, to form an opinion on the report and how it wishes to follow up the results and conclusions of the evaluation.
The aim of such an evaluation will be to see whether the approach taken can improve public health protection nationally, in particular, by controlling the quality of products taken by large numbers of the general public, and whether the new prevention strategies can limit use, stem revenue flows and the growth of organised crime, free up capacities and resources for reducing supply and combating organised crime, and reduce the contact between users and criminal circles that has, until now, been unavoidable. In fact, the current situation is not satisfactory for the reasons set out above and it would, therefore, seem fair, and indeed necessary, for the government to work towards finding solutions that are more likely to achieve the desired goals, based on scientifically valid data.
The scientific evaluation will be based on a baseline analysis of the current situation, during the period prior to the implementation of the national pilot project. The baseline data will then be supplemented by periodic analyses for the post-implementation period, in close collaboration with interdisciplinary experts, in order to 1) determine whether the national pilot project scheme is in line with its indicators and targets, 2) monitor emerging trends and their impact on public health, including changes in cannabis use and use-related behaviour, and 3) acquire new evidence-based knowledge.
In order to evaluate and monitor the impact of the national pilot project, six core targets with first, second and third priority indicators for evaluation and monitoring were selected. These were identified mainly by the working group through an extensive literature search and in collaboration with the EMCDDA in order to assess the drug situation and the potential impact of different legal and regulatory changes.
Each indicator associated with one of the six targets was assessed to see to what extent national data and information sources are currently available, the need for international data (EMCDDA, UNODC, etc.), as well as the timeframe for data collection (short, medium or long term) and its relevance in terms of achieving the future regulation’s objectives. The following non-exhaustive list of key epidemiological indicators is proposed:
- Identifying and monitoring factors associated with cannabis use, including psychosocial motivations and determinants e.g. risk perception, social attitudes and norms, socio-economic factors and mental health disorders
- Identifying and monitoring the prevalence of cannabis use and patterns of use among the general population, including vulnerable populations (e.g. groups with low socio-economic status, young people, those experiencing discrimination as a result of their gender, individuals with psychiatric co-morbidity (especially psychotic), etc.)
- Monitoring the prevalence of high-risk cannabis users
- Monitoring treatment provision and the proportion of high-risk cannabis users (cannabis as the main product) entering treatment, both in terms of access and treatment outcomes
- Identifying and monitoring changes in usage and possible impacts (including negative impacts) associated with the prevalence of use of other controlled and regulated psychoactive substances (including alcohol, tobacco, medicines and illicit drugs such as opioids)
- Assessing and monitoring morbidity and adverse effects associated directly and indirectly with cannabis use
- Collecting data and monitoring healthcare use directly and indirectly related to cannabis use (e.g. number of medical emergency episodes and hospital admissions related to cannabis use)
- Identifying and monitoring the social (family, professional, legal) and economic (loss of productivity, employment, school drop-outs, etc.) consequences of cannabis use
- Identifying and monitoring the consequences of the redeployment of policing activity
These indicators, in line with the objectives of the pilot project, will help to provide objective and reliable informationon cannabis use, its determinants and consequences in order to assess trends and developments in the supply and demand for cannabis. This work will make it possible to conduct a needs analysis to facilitate the development of targeted policy measures, including public health and public order intervention programmes.
The scientific evaluation will require one or more national mixed-method studies to collect data relating to the selected epidemiological indicators. For example, a general population survey (GPS) specifically dedicated to drug use and perceptions should be set up. The data currently available do not allow for a sufficiently nuanced assessment of the behaviours and perceptions associated with drug use prior to any change in the current regulatory framework, nor do they allow for measurement of the resulting effect on these indicators.
A general population survey could, therefore, cover and assess a large number of indicators. One example is the indicator of prevalence of cannabis use in the general population, for which measuring different rates of prevalence of cannabis use, including lifetime prevalence, past year prevalence and last month prevalence, is recommended. Analysis of non-use, past use and current use will make it possible to identify “new users”. The impact of usage will be one of the key indicators for steering and adjusting the planned policy. Other variables to be considered are socio-demographic factors, age at which cannabis use starts, frequency of use, psychosocial factors, etc. The general population survey should be supplemented by targeted studies that provide more detailed data on current cannabis users and (future) growers, e.g. cannabis users’ habits, quantities taken, usage patterns (including methods of taking cannabis), type of product taken (CBD-dominant/THC-dominant), intentions to grow cannabis plants at home, sources of cannabis acquisition (legal versus black market).
Establishing a representative general population survey supplemented by targeted studies will boost the availability of national data and statistics on the drug situation. The information gathered will facilitate study of the drug phenomenon, understanding of the impact of drug-related policy changes, identification of priorities and better planning of responses. Lastly, the general population survey will support the EMCDDA’s key indicator on prevalence and patterns of drug use, which makes it possible to collect and interpret harmonised and high quality European data.
This survey will require a nationally representative probability sample of people aged 15-64 and residing in Luxembourg. EMCDDA guidelines and European model questionnaires will be used to develop the questionnaire.
The evaluation studies will help to establish a baseline of specific indicators that are relevant in the context of the yet-to-be-implemented cannabis regulations. For example, it will be necessary to estimate consumption patterns and habits, motivations, attitudes and perceptions of risk, supply behaviour, and the prevalence of cannabis-related addictive disorders.
In addition, it is important to monitor trends in supply reduction indicators and the market for illegal psychoactive substances, including the number of cannabis seizures, quantities seized, street prices, types of cannabis products seized, THC concentration and contaminants in cannabis products seized in Luxembourg.[1] In addition, judicial and penal measures will be monitored, including the number of summons (arrests and charges) for cannabis-related offences. The number of fatal and non-fatal road accidents and cannabis driving offences will also be assessed.
Wastewater analysis can provide an additional source of data to qualify, or even validate, the survey data.
In addition to analysing the impact on public health, assessing the impact, before and after the pilot project, from an economic perspective is recommended. The economic impact assessment will focus on health economics approaches and a cost-of-illness study. This study will include, among other things, the costs to the health sector (direct costs), the value of lost productivity (indirect costs), and intangible costs.
Finally, a process evaluation of the national pilot project for legal access to cannabis for non-medical purposes should be considered. This evaluation will determine whether the different components of the pilot project were carried out as planned (fidelity) and whether its objectives were achieved. The process evaluation will generally review stakeholders’ experiences and help to determine which elements of the new pilot project are working well in practice, how well the pilot project is achieving its objectives, and which elements should be modified for improvement.
Evaluation of all aspects of the situation before, and after, the implementation of the pilot project will provide new scientific, theoretical and practical knowledge about cannabis use and regulation. The pilot project and its outcomes should be subject to ongoing monitoring and interim evaluations.
This evaluation process should be accompanied by a national research strategy, possibly in conjunction with international partners. In this way, Luxembourg will contribute to the international scientific community’s efforts to advance knowledge of all aspects of cannabis and to expand the scientific literature on the subject, which is still lacking. This approach will help to develop intervention programmes (preventive, educational, behavioural, psychological) based on scientific protocols and evidence.
[1] N.B. Seizures are not a particularly useful measure of the size of the black market. They are likely to be, above all, a measure of policing activity rather than market size, and the lessons to be learned from them may be distorted by a small number of significant seizures over a period of time.
The importing of cannabis is currently not a viable option. It will therefore be necessary to, right from the outset, plan for the establishment of a national production and marketing chain; given the current lack within Luxembourg of infrastructure for and experience of cannabis cultivation and production within a legal and controlled framework and environment, this looks likely, at the moment, to be a long-term undertaking.
It is recommended that a national control agency for that production and marketing chain be made responsible for oversight of the country’s production and producers and for the purchase of domestically produced cannabis. That option seems the wisest choice with a view to preventing companies’ profit-seeking from conflicting with the primary public health goal of reducing the negative side effects of cannabis use among the population at large. This national agency must be able to ensure the production of enough varieties of cannabis to prevent users from turning or returning to the black market.
During the establishment of the legal framework regulating production, it will be important to conduct a market analysis and determine whether the offering will meet users’ needs, in order to avoid over-/underproduction, or even a negative impact on changes to the ways in which the drug is taken. This goal could be achieved by limiting the number of production permits issued and/or a producer’s total permitted output. In addition, such a measure will contribute to mitigating the risk that legally produced cannabis could be diverted onto the black market.
On the basis of these considerations, it is proposed that producer companies be granted a maximum of two production permits and be able to acquire no more than one permit for a single production site. In order to be able to apply, companies will have to meet the quality requirements laid down by the authorities and the eligibility conditions set out in the specification. The permits will authorise the growing, processing and distribution, under certain conditions, of cannabis for non-medical purposes.
In view of the estimated number of potential users and of the small size of Luxembourg territory, it is estimated that two production sites will be able to meet domestic needs. Since the sustainable and guaranteed production and supply of cannabis for non-medical purposes is a key element of the later stage of the pilot project, this stage must not start until the legal framework regulating the production of cannabis for medical purposes is in place.
The production of cannabis for medical purposes is particularly important as part of a holistic and proactive approach, since the related legal framework being in place will therefore be a precondition for starting the subsequent stages described in the pilot project of legal access to cannabis for non-medical purposes.
The legal framework regulating production of cannabis for medical purposes will therefore serve, subsequently and after the related legal framework is in place, as the regulatory, administrative and logistical basis for establishing the production of cannabis for non-medical purposes.
2.5.1 Varieties of product
It is important to offer a varied range of products on the legal market, in order to meet users’ demand. The varieties of product that may be sold should be set out in the specification for a public tendering procedure relating to the allocation of production permits.
The products to be included must be decided on the basis of what is currently available on the black market and of the risks associated with using different varieties of cannabis. Those risks are closely linked to THC and CBD concentrations, and strongly influenced by the method used to take the drug and the amount taken.
Initially, a range of cannabis flowering-tops and resin products is being considered. Nevertheless, it seems appropriate to supply dispensaries with a range of cannabis varieties (several THC/CBD ratios and terpene profiles) and of appropriate THC and CBD concentrations, in order to ensure the lowest possible probability that users, unable to find the desired variety for sale legally, will turn or return to the black market.
In addition, since certain hybridisation and extraction techniques now make it possible to produce plant varieties or derived products containing very high THC concentrations (e.g. butane hash oil), the varieties and resins supplied by producers must meet the criteria laid down in the specification. The production and sale of pre-rolled cigarettes (joints), containing either tobacco and cannabis or just cannabis, must be prohibited.
2.5.2 General requirements for the producer to meet
It is recommended that producers should meet the following minimum criteria (non-exhaustive list):
- The producer must draw up a project proposal covering growing operations, post-harvest facilities, quality checks, quality-management system and the cannabis varieties (e.g. THC/CBD ratio and terpene profile) that it wishes to grow.
- The producer must guarantee the product quality standards – which have yet to be set out – throughout the production chain (growing, packaging, storage, etc.).
- The producer is responsible for security measures, in particular the completely secure storage of the cannabis, and must ensure a safe and healthy work environment.
- The producer must undertake to use exclusively the tracing software provided by the control agency, as defined in item 7, enabling the route taken by each finished product to be traced, so that the closed cannabis production chain can be properly monitored.
- Cultivation, drying and packaging of the product must take place on the same site, in order to avoid any unnecessary transportation.
- The producer must undertake to make every effort to prevent criminal involvement in the cannabis production and marketing chain and to cultivate no cannabis other than that which is to be sold at the dispensaries authorised under the national pilot project.
- The producer will not be permitted to sell online or deliver to customers’ homes.
- Every available resource is to be brought to bear to prevent the exporting of cannabis for non-medical purposes.
- The producer must meet stringent reliability requirements: the operator, manager and staff must exhibit a high degree of integrity, which will be checked in cooperation with the competent authorities; the THC and CBDcontent allowances of the dry weight – at a given percentage, to be determined – must be clearly marked and observed.
- The production of cannabis-derived products whose THC content deviates in a significant way – which has yet to be defined – from the level stated or required in the regulations should be considered a serious breach of the conditions for granting of the permit.
- Producers must demonstrate that measures are in place to make it possible to proactively avoid producing surpluses and to enable secure storage of surpluses in a way that safeguards their quality, for instance by means of refrigeration. These measures are necessary in order to appropriately respond to the ebb and flow of the Luxembourg market, which is intrinsically limited.
- Producers must, upon the national control agency’s request, grant inspectors access to representative samples of a batch of cannabis, so that it can be sent to an independent and state-approved laboratory for testing.
- Producers must, using specific methods yet to be determined, destroy:
- a) The compounds or derived products from a batch of cannabis or those resulting from a batch that does not meet the quality control requirements
- b) Stock remaining unsold once an expiry date has passed
- Producers must meet certain requirements favouring production sites that will adequately meet the climate goals in respect of renewable energy sources set out in the 2018-2023 coalition agreement. Thus, the specification will lay down as-yet undetermined requirements in respect of self-sufficiency in renewable energy, and energy-efficiency and emission-reduction measures.
- The conditions under which producers operate and set up business must be agreed with the competent authorities (environmental impact, water supply, wastewater disposal, etc.).
- Producers must be registered with the appropriate trade association.
2.5.3 Storage and quality checks
The working group considers it important to put safeguards in place to ensure both the quality (of refrigerated cannabis stockpiles, for instance) and the security of the product while it is being stored.
Before the pilot project is up and running, it is proposed that each production site ensure that it has a back-up supplyequivalent to one production cycle for all varieties cultivated. Provision will need to be made for an initial stage and a market-maturity stage to adapt suitable back-up supplies.
In addition to the quality requirements for growing, independent quality checks and cannabis analyses should also be organised. This makes it possible to conduct checks on whether the product meets the quality (contaminants, pollutants, plant protection products, plant growth regulators, etc.) and concentration (THC and CBD) requirements. It is important that, in order to prevent any conflicts of interest, a certified independent body be made responsible for these quality checks. In parallel, it will also be necessary to guarantee that the relevant agricultural best practice is observed.
2.5.4 Product quality standards
The quality of cannabis for non-medical purposes to be produced by the selected producers should meet the quality standards, which will be laid down in a grand-ducal regulation.
It is proposed that producers be required to produce cannabis of quality compatible with public health goals and with the objective of gradually eroding the black market. One of the results of this requirement is that quality will be uniformly beyond reproach and that there will be no consumer-protection disputes consisting of criticisms that products are of inferior quality to those found on the black market.
Production and quality standards should be drafted to incorporate the following points (non-exhaustive list):
- Clearly defined government standards setting upper limits, or undetectable levels, of plant protection products, contaminants and pollutants:
- Prohibition against using any plant-protection products (pesticides, fungicides, etc.) and plant growth regulators: It is proposed to prohibit the use of these producers and, if necessary, to require producers to use organic methods. Certification that meets the requirements for organic farming standards is recommended.
- Production that meets the requirements of the food industries’ quality assurance systems, where that proves beneficial for producing cannabis for non-medical purposes:
- Consider the possibility of partially or fully applying good agricultural and collection practices (GACP). They contain regulations on food safety, packaging, and working environment and conditions;
- Set out a quality management.
2.5.5 Container and packaging
The producer should ensure that the container meets the following requirements and has the following characteristics (non-exhaustive list):
- Being airtight
- Having a childproof catch
- Not looking attractive to children
- Ensuring that the product is properly preserved
- Being sealed once the product is ready to be dispatched to the dispensary
- Being sealed in such a way that it cannot be opened without damaging the seal but that it can be closed again
- Being uniform and containing an amount weighing the same as one of the measures in which cannabis is normally sold (1, 3 or 5 grams)
All packaging should be identical and the “plain packaging” principle must be applied and respected.
The container label should also display the following information (non-exhaustive list):
- Product name
- Product type
- Producer’s name and contact details
- Quantity in grams
- THC and CBD content and ratio: the THC and CBD content allowances and the ratio of the two substances must be stated on the products sold, accompanied by a risk score represented by a colour code
- Universal THC symbol
- Batch number
- Use-by/expiry date
- Storage recommendations
- Unique code for the monitoring and tracking system
- QR code with practical information for users (e.g. analysis results, detailed information on, for instance, the presence of terpenes and the cultivation method)
- Quality label proving that the product has been checked by an official body
- Made in Luxembourg label
The container should also bear the following warnings, on a rotational basis (non-exhaustive list):
- “Contains cannabis”
- “Keep out of the reach of children”
- “Smoking cannabis is the most harmful way to take it”
- “Do not drive a motor vehicle or use machinery while under the influence of cannabis”
Instructions, in French, German, English and Portuguese, should be enclosed with the container, including the following information (non-exhaustive list):
- Recommended method(s) of administration
- Contra-indications
- Adverse effects
- Precautions for use
- Drug safety monitoring contact details
- Information on accessing treatment services
- The following warnings:
- “Do not smoke cannabis, pure or with tobacco.”
- “There may be a delay of two hours or more before intoxicating effects occur.”
- “Women who are pregnant, breastfeeding or intending to become pregnant are particularly at risk from this product.” Possibly add a pictogram of a pregnant woman in an interdictory circle.
- “Cannabis use can lead to substance abuse and addiction.”
It is recommended that the packaging developed and marketed in accordance with the above requirements also comply with the principles of the circular economy. The specific criteria to meet should be laid down in the specification for the production permit.
The distribution chain, from producers to dispensaries, should be organised by the producers and be transparent, so that it can be monitored and so that no cannabis can end up in criminal hands. The eligibility criteria for hauliers will be specified in the regulations.
The number of stops during transportation must be kept to an absolute minimum, in order to reduce all risk that cannabis will disappear from the closed distribution chain.

It is proposed to incline towards a public body for operation of distributors of cannabis for non-medical purposes. The intention is to avoid the risk that the marketing of cannabis products will, even with strict legal controls, bring companies’ profit-seeking into conflict with the primary public health goal of reducing the negative side effects of cannabis use among the population at large.
The working group takes the view that publicly owned dispensaries are more likely to comply with other regulatory limitations imposed by the state and are best placed to ensure both sales and qualified staff who will, to the best of their ability, strive for the achievement of the goals being pursued as part of the pilot project.
Publicly owned dispensaries have a number of advantages:
- Independent, strategic identification of the dispensaries’ specific locations
- Dispensaries’ swift, harmonised and simultaneous adaptation in the event of potential changes being made during the pilot project
- Ease of implementation of recommendations pertaining to, among other things, prevention and health promotion
- Lack of commercial pressures and their negative side effects
- Lack of competition between dispensaries
- Easier price setting and adaptation in response to the reactions and commercial strategies from the black market
It is therefore proposed that 14 dispensaries be established, at least during the initial stage. Item (a) of this chapter sets out the exact distribution of these dispensaries, on the basis of resident population per canton. In order to prevent “cannabis tourism” for non-medical purposes within Luxembourg, that distribution will have to be fairly even, in terms of both geography and population. To a certain extent, the locations of the 14 dispensaries will also be partly determined on the basis of population densities by workplace and of commuting routes.
The dispensaries must be used exclusively to sell cannabis for non-medical purposes. The state, or companies duly licensed by it, will be the exclusive suppliers of the dispensaries, at a price set by the state. That price will include packaging and secure transportation to the dispensaries. No other suppliers of cannabis for non-medical purposes will be tolerated; should other suppliers be used, civil and/or criminal proceedings will be brought without delay.
The only people eligible to buy cannabis for non-medical purposes will be residents 18 years of age or older. Customers’ right to buy will be verified using an information system provided by the Luxembourg Government IT Centre (CTIE). This system will consist of a secure terminal, a system for scanning the bar-codes included on the packaging and the related systems, such as the secure link to the National Register of Natural Persons (RNPP), the specific software application for entering the quantities bought by the customers and for checking, in real time, whether the monthly volume per resident of legal age has been exceeded. No other information system or software may be used on the terminal provided by the CTIE. The CTIE will perform preventive and corrective maintenance and any operational error must be reported to it as swiftly as possible. Telephone and remote support will be available during the dispensary’s business hours. In order to minimise the risk of computer system intrusion, the selected economic operators must have secure telephone and Internet connections. The state, through the CTIE or one of its specialist suppliers, reserves the right to conduct penetration tests, scheduled or unannounced, in order to check the security of telephone lines and Internet connections. These tests will take place before the above-mentioned terminal is installed and at least once per year.
Customers must be kept safe in the dispensaries and the property that the points of sale contain must be kept secure. At the least, a guard must be present in the dispensary during its business hours and at its closing time. The goods must be placed in strongrooms, with appropriate hygrometry- and temperature-control systems. Customers will be able to pay for their purchases by any legally permitted means. The dispensaries must, consequently, make provision for a cash-in-transit service, in order to prevent the accumulation of large sums of cash that, combined with the value of the stock of cannabis for non-medical purposes, could make the dispensary a target for criminals, including organised crime groups. In that connection, the specification will set out minimum and maximum levels of stock of cannabis for non-medical purposes. In the specification, the state will establish the type of premises that may house dispensaries of cannabis for non-medical purposes and all the details relating to making those dispensaries secure. Dispensaries should be open from 12.00 to 20.00 Monday to Saturday, excluding public holidays.
A dispensary may only be officially opened once it has been fully checked by the competent state services. Such checks, unannounced or regular, will also be conducted on the subcontractors of the selected economic operators, such as security or cleaning firms. In addition, other unannounced checks will be conducted on, for instance, premises security systems, the quality of storage for cannabis for non-medical purposes and compliance with dispensaries’ obligations.
There will be checks on the presence of a sufficient number of prevention and awareness-raising documents. In that connection, the state, or an authorised organisation, will provide the selected dispensaries with all the materials necessary for carrying out indispensable prevention and awareness-raising assignments. The employees of the selected concessionaires will, before the dispensary is opened, be duly trained on the best way to carry out those assignments. A dispensary will need to be staffed by at least three people at all hours of the day, in order for all prevention, awareness-raising, sales and administrative assignments to be carried out.
2.7.1 Geographic distribution of dispensaries
The geographic distribution of dispensaries is to be settled by a competent institution on the basis of criteria; both the institution and the criteria are yet to be determined. In general, it is recommended to limit the number, density (geographic and population) and type of the dispensaries.
In the context of the national pilot project, it is proposed to establish one dispensaries in each of the following cantons, in order to ensure national coverage representative of the population density.
- 1 dispensary in the Canton of Diekirch
- 1 dispensary in the Canton of Grevenmacher
- 1 dispensary in the Canton of Capellen
- 4 dispensaries in the Canton of Luxembourg
- 4 dispensaries in the Canton of Esch-sur-Alzette
- 1 dispensary in the Canton of Mersch
- 1 dispensary in the Canton of Remich
- 1 dispensary in the Canton of Redange
Following the national pilot project, it will be possible to adapt the number of dispensaries to demand.
As regards the distribution of dispensaries, it will also be necessary to consider the fact that many people are able or obliged to make purchases in the canton where they work, not necessarily their canton of residence.
In relation to the location of dispensaries in the selected cantons, consideration must be given to laying down some requirements in respect of the conditions for setting up a dispensary (for instance, required distances from educational establishments, care model, easy access for people with reduced mobility, etc.).
2.7.2 Obligations that dispensaries must meet
It is recommended to rule out the options of online sales and home deliveries.
All dispensaries should meet the following requirements (non-exhaustive list):
- The products offered must be bought exclusively from domestic producers approved by the public authorities.
- The dispensary must not hold more than the permitted stock on hand.
- Each dispensary should assess its stock on hand on the basis of need.
- The dispensary must meet its obligations as regards information on the product and on prevention.
- The dispensary may only sell the permitted cannabis products. Dispensaries must check whether they are entitled to sell cannabis accessories.
- The sale of alcohol is strictly prohibited.
- The dispensary is responsible for storing products in a way that preserves their quality, i.e. in a temperature- and humidity-controlled environment.
- The dispensary must ensure that its customers can use cash or bank cards to buy cannabis products.
- The dispensary must ensure secure storage of its products and guarantee a safe and healthy working environment.
- The dispensary must meet the sales-quality requirements.
- The dispensary must meet stringent reliability requirements.
- The dispensary must register all customers and check their entitlement to buy cannabis.
- The dispensary must ensure that the maximum quantities delivered every month are not exceeded. Taking into account the national situation, a monthly limit of 30 grams of dried cannabis per customer is recommended.
- The dispensary must ensure, by means of a joint computer system, that the daily limit of 5 grams per customer is not exceeded.
- The dispensary must ensure that no cannabis is used on its premises.
- The dispensary must do everything in its power to ensure that its activities do not cause problems (noise, litter, etc.) in its vicinity.
- The dispensary must respect the perimeter established in the specification in respect of proximity to schools, youth clubs, care homes, nursing homes, etc.
- The dispensary must undertake not to market or offer pre-rolled cannabis cigarettes (joints). The sale of tobacco, including tobacco-related accessories, will be prohibited.
- Customers must be encouraged to give preference to inhaling cannabis vapours by means of vaporisers and to cut back on smoking cannabis (pure or mixed with tobacco). Dispensaries should therefore be authorised to sell vaporisers.
- The dispensary’s staff may not process or handle the products intended for sale in any way. This prohibition does not apply to the presentation of samples of no more than 20 grams, made available by producers so that clients can evaluate the products for sale.
- The dispensary must ensure that no one opens a product’s packaging on the premises.
- Non-residents and people under 18 years of age will be prohibited from accessing dispensaries.
- Dispensaries must have limited business hours and days. It is recommended that dispensaries be open Monday to Saturday, 12.00 to 20.00, excluding public holidays.
- Dispensaries must not display advertisements promoting or encouraging cannabis use. Economic operators must not participate in any activities promoting and advertising cannabis for non-medical purposes, including the sponsoring of events and participation in events, conventions, trade fairs, etc. relating to promoting cannabis and products derived from it. The purpose of a dispensary must not be apparent from the outside, in other words they should not display any advertising that could encourage cannabis use.
- The dispensary may, however, very visibly display on its premises materials provided by the state or an authorised organisation, such as health warnings, educational literature and the contact details of consultation and therapy services.
- The dispensary is required to clearly explain, on its premises, how and why customers’ personal that is recorded will be processed, in accordance with the data protection legislation in force.
2.7.3 Stock management in the dispensaries
- Each dispensary is responsible for recording, by means of the allocated unique code, all products received.
- The dispensary is not entitled to hold more than the permitted stock. The stock of cannabis necessary depends on the average quantity sold; it should be borne in mind that these averages can vary depending on the dispensary and, in particular, on its location. It is recommended to set the maximum stock level for each dispensary at such a level that the cannabis must not be delivered more than once per day; in other words, the stock should be sufficient for at least one day and no more than six given business days.
- The security conditions (strongroom with monitored entrance) are to be determined.
2.7.4 Role of sale price
It is as difficult as it is crucial to set a fair price for the varieties and products sold by legal dispensaries. The goal is to make black market products less attractive, but without encouraging members of the public to use or even to start using legally sold cannabis. Discussions with representatives of other countries where there is experience of this should help a solution to this problem to be found, although the unique situation of Luxembourg (e.g. purchasing power, current prices on the national black market) should be borne in mind.
The national control agency should set the price, which should be neither too high nor too low. Too high a price could encourage users to buy cheaper products on the black market. As far as possible, the price should be guided by the black-market price. A regular evaluation will be necessary. The mechanism for setting prices should offer the flexibility necessary for it to be adjusted in line with changes on the black market.
In-depth analysis of the applicable taxes must be carried out. Where applicable, the taxes will be guided by EU legislation and the Belgium-Luxembourg Economic Union Convention. The taxation level is a variable relevant in terms of public health policy and should be the one that will enable achievement, to the greatest extent possible, of the goals being pursued (see chapter I.3).
As set out in the coalition agreement, the working group recommends that “In the investment of the revenue generated by cannabis sales, priority should be given to prevention, awareness-raising and treatment in respect of the huge numbers of addicted people”. Nevertheless, public health interventions, administrative work, enforcement action and research must be funded according to need, rather than being dependent on sales.
A lower price could initially help to avoid the repeating of experiences observed in some other countries, where the high price and scarcity of legal products benefitted the existing black market.
The price strategy must enable the competent authorities to discourage the use of cannabis with high THC content, which represents an increased health risk. Therefore, the option of a progressive and variable price that increases with THC content should be considered.
Maximisation of tax revenues must not be considered a goal in itself. Tax revenues must ultimately be considered an additional benefit that makes a positive contribution to investment in public health.
[1]Kugener, T., Berndt, N. & Seixas, R. (manuscript in preparation). Enquête Européen sur les Drogues au G.D. de Luxembourg 2021. Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health: Luxembourg.
2.8.1 National control agency
Under Articles 23 and 28 of the United Nations Single Convention on Narcotic Drugs of 1961, as amended by the 1972 Protocol, of which Luxembourg is a signatory, any party to the Convention that permits the cultivation of the cannabis plant for the production of cannabis or cannabis resin for industrial purposes (fibre and seed), is required to establish and maintain “one or more government agencies” to apply the system of controls as provided for in article 23 of the Convention in respect of control of the opium poppy.
Therefore, the establishment of a competent government agency is required under international law. It will be necessary to clearly define the ministry to which the national control agency reports, along with the agency’s make-up and duties, and to establish the legal basis required for its setting-up and operations.
2.8.2 Governance
It will have to be decided which public bodies will be jointly performing the role of national control agency for the cannabis production and marketing chain. Additional resources will have to be allocated, if the various tasks involved in these control and regulatory duties are to be adequately performed. A monitoring committee should be established, in order to support and supervise development and to ensure that the goals being pursued, as described in chapter I.3, are achieved.
2.8.3 Distribution and duties
The national control agency’s duties might be distributed between several public bodies, which will be determined gradually in due course.
It is proposed to develop a computing platform[2] that will enable the whole journey of a cannabis-derived product from producer to user, via the dispensary, to be monitored. By recording every stage in the journey and the product’s status, this system will make it possible to trace the origin of every cannabis product and the route it has taken, so that the closed cannabis production and marketing chain can be properly monitored. Products will be assigned a unique code, so that the batch can be identified. In Canada and several US states, the seed-to-sale system is already in use and has proved reliable.

2.9.1 At the production level
- Producers must register their products once they have been packaged, so that their stock can be tracked.
- Products must be registered before transportation and during delivery to the dispensary, in order to guarantee that no products disappear in transit.
2.9.2 At the dispensary level
The working group recommends that the architecture[1] of the tracking system and of the national database make it possible to trace the product at all times and to check whether the customer is entitled to enter the dispensary and buy the product.
Dispensaries will have the role of data processor and must therefore strictly adhere to the duties set out by the data controller, which will be the national control agency.
The identification of customers in dispensaries requires vendors to register customers in the system that has been put in place and is supervised by the national control agency.
The system must have a connection in the background to the National Register of Natural Persons (RNPP), so that it can be verified whether the customer is both a Luxembourg resident and the required age to enter a dispensary andbuy the product.
In addition, the must have a second connection to the central database, in order to enable it to check whether the customer has exceeded the permitted monthly quantity.
Vendors will not have direct access to the various database mentioned above; the system will only allow them to check whether the conditions precedent have been met or not. Vendors may only go ahead with selling the product if all three conditions have been met. Vendors must therefore scan each product (packaging) sold, in order for each sale to be recorded in the national database.
All personal data will be pseudonymised and held in the national database for a maximum of two years. The national control agency will not be able, at any time, to discover the customer’s identity.
A body with the role of trusted third party must be named and will be responsible for pseudonymising all data before it is sent to the competent authority.
The following personal data will be recorded, for a maximum of two years, in the national database:
For each product:
- product name
- product type
- producer name
- quantity in grams
- batch number with use-by/expiry date
- unique code and tracking history
For each sale:
- customer’s pseudonym
- customer’s age
- product’s unique code
- customer’s sex
- canton of residence
- dispensary’s location
In terms of data protection management, it is proposed that the process of selling cannabis for non-medical purposes follow these stages:
- Potential buyer visits dispensary.
- Buyer presents identity document to vendor in dispensary.
- Vendor checks that the appearance of the potential buyer matches the person shown (in the photo) in the presented identity document.
- Once the buyer’s identity has been checked, the vendor encodes the potential buyer’s full name and date of birth in the dispensary’s software.
- The encoded details are sent to the trusted third party via the dispensary’s terminal.
- The trusted third party checks the received data in the RNPP and collects the data necessary for checking the eligibility criteria (age and country of residence).
- The trusted third party generates a pseudonym for the checked person.
- The pseudonym and the data necessary for checking eligibility criteria are sent by the trusted third party to the data processor via the dispensary’s monitor.
- The data processor checks the information received against the eligibility criteria and sends the approval or refusal of the sale to the pseudonym in question to the dispensary’s monitor.
- The seller receives an approval or refusal message on the dispensary’s monitor.
- In the case of approval, the vendor completes the sale and sends the related data to the data processor via the dispensary’s terminal for recording in the customer-monitoring database.
It is recommended that the pseudonymised data be retained for two years and then be anonymised. The data will be used to conduct statistical research. The pseudonymisation may only reversed by the trusted third party and doing so will require an injunction.
[1] See Annex 2.
[2] As part of the process of drawing up this draft concept note, the Directorate of Health conducted an assessment of the data-protection impact of the processing of personal data.
2.10.1 At the production stage
The following steps should be taken in order to prevent any cannabis from, for instance, ending up in the hands of criminals:
- Secure production sites and facilities, with particular attention on storage
- Rigorously check the plants being grown (e.g. by counting and labelling the plants, by weighing products at several points, by sealing packaging, etc.)
- As far as possible, grow, dry and package cannabis in a single place, in order to minimise stops during transportation
- Ensure that the principles laid down in Chapter II.3 (“Production”) are respected
2.10.2 At the transportation stage
In risk management terms, this is the most vulnerable stage, owing to the risk that the vehicle will be stolen or robbed The producer is responsible for distribution and must, in order for sufficient security criteria to guarantee a closed cannabis production and marketing chain to be integrated, establish the following:
- Secure, trackable transportation in an unmarked vehicle with notice given of the delivery
- Status, equipment and training of the driver’s assistant
- Conditions of loading and unloading
2.10.3 At the sale stage
Dispensaries must ensure a secure working environment and secure storage. The following conditions must be met:
- Storage in a restricted-access strongroom
- Presence of a security guard
2.10.4 Production and sale staff
Those employed in production and sales must meet stringent reliability requirements: the operator, manager and staff must exhibit a high degree of integrity, which will be checked in cooperation with the competent authorities.
Provision will be made for administrative and criminal penalties.
The current legislation on drugs in Luxembourg is based on the Act of 19 February 1973 on the sale of medications and the combating of drug addiction, as amended. This piece of legislation regulates the production, use, possession, delivery, sale and trafficking of controlled drugs. The Act of 27 April 2001 materially changed the legal framework in Luxembourg, by introducing, for the first time, differentiation of penalties on the basis of the types of substance involved. As such, there is cannabis-specific legislation already in place and it is partially distinct from that relating to other illegal drugs. Since 2001, there has been no provision for custodial sentences for merely using cannabis or possessing it for personal use; only criminal fines may be imposed. However, the sale of cannabis, and its importation, exportation or use, when accompanied by aggravating circumstances, are subject to severe criminal penalties.
In the criminal policy followed since then, a pragmatic approach to this matter has been adopted, with a focus on treating users, rather than punishing them. In line with that policy, therefore, those who merely use cannabis already enjoy a more favourable legal regime.
As part of current youth protection policy, a range of psychosocial and therapeutic support offerings are now made available at the national level to young people, their families and the affected institutions in cases of the use of legal and illegal psychoactive substances by someone under the age of 21. Under the Act of 1973, as amended, the public prosecutor has the right to end any proceedings against addicts who agree to undergo a drug treatment programme. In 2001, a legal framework was also introduced for substitute drug treatments for addiction; such treatments had previously been tolerated but illegal. As part of the legislative work towards implementation of this concept note, the arrangements need to be further refined, in order to duly take into account the pilot project and the reform of the criminal law in respect of minors.
The effective operation of the system to be implemented in accordance with this concept note requires a coherent package of effective, adapted, proportionate and dissuasive penalties. To that end, use will be made of both administrative penalties – such as administrative fines or the revocation of concessions and permits on the order of the national control agency – and criminal penalties handed down by the competent criminal courts.
2.11.1 Administrative penalties
The following is a non-exhaustive list of administrative penalties:
- Administrative fines in the event of failure by producers or dispensaries to meet their obligations, for instance by holding quantities in excess of the permitted maximum; these fines could be doubled in the event that such a failure is repeated
- Closure (temporary or permanent) of a dispensary or production premises
- Revocation by the national control agency of the permit of a dispensary or production premises
- Administrative fines in the event of a person of legal age possessing quantities of cannabis in excess of the permitted maximum of 5 grams or using cannabis in public
- a ban (temporary or permanent) on accessing points of sale
2.11.2 Criminal penalties
Given that the pilot project of access to cannabis for non-medical purposes will risk inciting criminal elements to make up, one way another, their lost profits, it is essential not to relax enforcement of the law in respect of narcotics, in particular as regards the illegal production, growing and trafficking of cannabis and other illegal drugs.
Public health and safety must be protected by means of strengthening the legislation and the actions taken to punish and respond effectively to serious cannabis-related offences, in particular selling cannabis in a way not permitted in law.
Selling on non-medicinal cannabis to minors or non-residents and sharing it with such individuals must be prohibited and subject to deterrent criminal penalties, including custodial sentences.
In the context of the bill implementing this draft concept note, all current criminal penalties will undergo a critical assessment, in particular those for breaching the prohibitions against the illegal sale, production and trafficking of cannabis (whether from the legal cannabis production and marketing chain or from elsewhere), with a view to the establishment of a coherent and appropriate set of related criminal penalties.
The government, municipalities, law enforcement agencies and competent authorities are responsible for monitoring and overseeing compliance with the rules in place and the legislation in force.
In general terms, the Act must include at least the following provisions:
- Permission for the possession, in private and public, of quantities of cannabis of up to 30 grams, exclusively in the sealed packaging of an authorised dispensary
- Permission for the possession, in private and public, of quantities of cannabis (or the equivalent) of up to 5 grams, sealed or unsealed
- Provision for the prohibition against possession of cannabis by people under the age of 18, even when it is available on the legal market; depending on the individual’s age and the seriousness of the offence, young people breaching this prohibition will be subject either to the provisions of the Youth Protection Act or to the Act establishing a criminal law regime in respect of minors
- Provision for wide-ranging inspection and seizure powers, including the right to access any premises in respect of which there are reasonable grounds to believe that an activity that could be governed by the Act is taking place, and the power seize and retain cannabis or any other item in respect of which there are reasonable grounds to consider related to breaches of the Act
- Provision for the prohibition against the use of cannabis, whether flowering tops or resin, in premises open to and/or serving the public; cannabis use will also be banned in premises where the smoking ban (tobacco or e-cigarettes) applies
For dispensaries, the intention is to impose the following obligations, failure to observe which is to be combined with appropriate administrative or criminal penalties:
- Prohibition against selling to any individual under 18 years of age
- Prohibition against selling to non-residents
- Prohibition against selling to legal entities
- Prohibition against selling amounts in excess of what is provided for in law
- Prohibition against selling illegal cannabis that is not produced domestically
- Prohibition against selling cannabis not contained in its sealed original packaging
- Prohibition against producers and authorised dispensaries from selling cannabis online
Mitigating circumstances should be considered in cases where the dispensary has taken reasonable measures to check a person’s age or place of residence, for instance, but that person presents fake or stolen documents, acts that are already criminal offences.
For users, the future legislation must prohibit commission of or intent to commit the following acts:
- Sale or giving free of charge to a non-resident by a person of legal age
- Sale or giving free of charge to a minor by a person of legal age
- Any form of inducement, by a person not permitted to buy cannabis on their own behalf, of another person to buy cannabis for them
- Sale or giving free of charge of cannabis to another person, even if that person is entitled to legally buy cannabis at an approved dispensary
- Use of cannabis in any non-private setting
- Possession in public by a person of legal age of a quantity of cannabis in excess of 5 grams that is not contained in its sealed permitted original packaging
- Crossing of the land, air or river borders of Luxembourg by a person of legal age with any quantity of cannabis
This list is not exhaustive from a legal perspective. Note that some acts are already subject to criminal penalties, such as using a fake identity document to impersonate another person.
Any person committing one of the above-mentioned acts in relation to or with a quantity of cannabis that clearly goes beyond private personal use should be considered a drug trafficker and will be subject to the applicable severe criminal penalties.
The working group considers it essential that the pilot project of legal access to cannabis for non-medical purposes go hand in hand with the development of existing measures relating to preventing the use of cannabis for non-medical purposes and reducing its potential health risks and harmful effects. The pilot project actually offers new possibilities and opportunities for developing prevention work, by making it easier to access cannabis users and facilitating the work of using prevention messages to inform them and raise their awareness.
In order to do everything possible not to make cannabis more attractive and thereby, potentially, increase smoking levels, complementary preventive measures will also have to be taken to counter the trivialisation and normalisation of cannabis and tobacco use, in particular among young people, in order to prevent undesirable effects on individual and public health.
Information and universal, selective and indicated prevention measures must start during primary education; reach children in their home and school settings and in their recreational activities; be routine and diverse; target both occasional use and the detection of high-risk use; make use of all the available tools and networks; and be specific to different age groups and other target groups.
Prevention strategy must be based on a holistic concept that goes beyond preventing and reducing risks related to the use and misuse of cannabis: it must promote general well-being and the development of skills in relation to cannabis use and of skills linked to managing the related risks.
It is essential to include young people; their parents; teachers, education staff and school management; their general practitioner; the representative of their local education authority; their tutors; and groups of their peers in prevention strategies, and to make use of all digital and other tools and media available for prevention and for offering those involved information and training.
In this regard, a crucial role is played by the National Addiction Prevention Centre (CNAPA), whose articles of association provide for, among other things, the drawing-up of a national concept note for systematic and structured prevention work and for implanting that concept note jointly with existing national and international organisations and institutions.
2.12.1 Communication and awareness-raising strategy
The pilot project of access to cannabis for non-medical purposes might bring about changes as regards the perception of risks and hazards linked to its use.
The working group therefore recommends developing, in close consultation with the public authorities relevantfor the target groups (e.g. the Ministry of Education, Children and Youth or the Ministry of Higher Education and Research), external experts and partners on the ground active in combating addictive behaviours, a complete and well thought-through communication strategy to provide information about the pilot project before its implementation. This will contribute to adequately informing target groups and other stakeholders about the rules and legal framework in place in respect of legal access and about the ability of each individual to make an enlightened and responsible choice. This communication will mainly take the form of public campaigns using the communication channels best suited to the target groups.
The strategy must address the properties of cannabis, its potential risks for users and those around them, and the characteristics of its various types, qualities and methods of use. The messages must be balanced, respectful and convincing for the main target groups.
The communication must also address adults in direct contact with young people, in particular vulnerable young people more at risk of high-risk forms of using cannabis (parents, teachers, employees of youth justice institutions, people working in the field of care for young people with mental disabilities). People working in the system – employers, teachers, law enforcement officers, healthcare professionals, etc. – will need information adapted to their specific roles.
A multi-year communication plan must be drawn up for each of the various target groups and must state which communication tools will be appropriate. This communication plan must include an action plan, coordinated with the various partners on the ground. A multiannual budget must be established, with a view to ensuring consistent communication.
The communication strategy must also cover the labels to affix to packaging for cannabis and products containing cannabis include health warnings based on scientific evidence, contra-indications, risk-reduction messages and information on accessing support services.
2.12.3 Prevention and education strategies
Messages for the attention of people choosing to use cannabis must be systematically disseminated, with the aim of reducing risk and potential damage.
Both before and after the pilot project of access to cannabis for non-medical purposes comes into force, it is essential to develop, in close consultation with external experts and services specialising in the field of addiction, even more prevention programmes based on and guided by scientific evidence.
The main challenge will consist of adapting these different strategies to target groups and contexts and of ensuring that they have solid foundations and sufficient coverage at the national level. Too few programmes of this sort are currently available to address these new challenges.
Several types of prevention strategy need to be considered, such as those targeting society as a whole (environmental prevention) or interventions targeting at-risk people (indicated prevention):
- Environmental prevention strategies to change the cultural, social, physical and economic environments in which people choose to use cannabis
- Universal prevention strategies targeting whole schools and communities, with a view to giving young people the social skills necessary to avoid or delay starting to use cannabis
- Selective prevention strategies targeting specific groups, families or communities that are at greater risk of becoming addicted to cannabis
- Indicated prevention strategies targeting individuals identified as presenting increased risk factors in respect of addictive behaviours
- Early intervention strategies intended to delay or prevent the use of psychoactive substances
Young people should be the priority targets for these measures.
Prevention programmes should be based in the best scientific evidence available and include multidisciplinary interventions in schools, focused on social skills and refusal skills, on informed decision-making and handling certain situations and on correction of certain widely held but incorrect beliefs about drug use.
In addition, interventions at the family level and structured health interventions should take place, along with counselling sessions and motivational interviewing. Prevention programmes in several settings, involving various specialisms and combining a number of approaches seem most effective. In this context, it is recommended to put in place guidelines in schools for setting up information and prevention sessions, not just about the potential risks and harm from cannabis use, but also about addiction in general. Likewise, guidelines should be put in place on how to respond to signs of abuse and addiction.
In addition, it would be desirable for schools to be able to call on a team of specialists to take preventive and prohibitive action on addictive behaviours in the broader sense (substances, screens, gaming, new media, etc.). For the purposes of national coverage, this team should be structured in such a way that each specialist covers several schools.
It is also important to target other vulnerable groups, such as pregnant and breastfeeding women, people with a personal or family history of mental health or people with a history of problems resulting from substance abuse.
In order to ensure the implementation of prevention strategies, training should be provided for the major players at the various levels of addiction prevention, in particular cannabis-addiction prevention. This training should be offered to stakeholders working with adolescents and other vulnerable groups (e.g. specialists involved in youth clubs, schoolteachers’ representatives, municipal administrators, etc.). This training should include subjects such as protection of minors, communication about cannabis use, addiction prevention, early detection of cannabis addiction, treatment options, etc.
Strategies intended to increase resilience, responsible and well thought-through risk management, (pycho)social skills and decision-making skills and other personal resources have proved to have beneficial effects.[1],[2],[3],[4]Supplementary studies examining the relevance and relative effectiveness of interventions intended to prevent and reduce cannabis use. Prevention interventions should be adapted to the stage of development of adolescents or of the target group and should involve the parents/family and peer groups, but also social networks.
2.12.4 Sales practices
It is important to incorporate preventing cannabis use, in particular among young people of legal age, into the stage when cannabis is being sold in dispensaries. Appropriately trained staff should be responsible for discharging this duty.
This training should be carried out by the national control agency or by its appointees. It must be conducted regularly, at least every two years, in order to keep staff’s skills up to date.
- Dispensaries’ staff must receive tailored training to enable them to advise and inform customers appropriately about how to use cannabis in the most responsible way that best minimises risk and harm.
- Dispensaries’ staff must have advanced knowledge of the health effects and risks of cannabis and must adequately inform customers about those effects and risks.
- Staff must be able to recognise the signs of abuse and addiction.
- Where a customer shows signs of high-risk usage, staff must be able to refer to appropriate information or services, such as an online platform where it is possible to interact in real time with addiction-care professionals.
- Dispensaries’ staff should be required to recommend or propose that users initially buy cannabis products with lower THC content and with a balanced THC/CBD content ratio, which has yet to be determined.
- Staff must be able to propose and explain the information materials that are available and clearly displayed in dispensaries.
- Staff must be able to suggest to customers they conduct tests on themselves, with a view to assessing their own usage level and its associated risks.
2.12.5 Customer information
It is important that all the information labels affixed to packaging for cannabis and products containing cannabis include evidence-based health warnings, contra-indications, messages on reducing potential and risks and harms, and information on accessing prevention and treatment services.
Some key messages should be communicated to users in parallel with those included in the instructions (non-exhaustive list):
- Rather than smoking cannabis, vape it.
- When using cannabis, do not mix it with tobacco.
- Do not use cannabis if you have a family history of mental illness.
- Do not use cannabis products with high THC content and low CBD content, since the latter seems to be able to partially counteract the psychoactive effects primarily derived from the THC contained in cannabis products. Try to choose cannabis products with high CBD content and low THC content.
- Only use cannabis in your free time and when you are felling well.
- Limit the frequency of your cannabis use.
- Do not use cannabis while pregnant.
- Do not use cannabis at the same time as other psychoactive substances, such as alcohol.
- Do not drive while under the influence of cannabis.
2.12.6 Prohibition of promotion, advertising and marketing
It is recommended to prohibit all activities promoting and advertising cannabis for non-medical purposes, including the sponsoring of events and participation in events, conventions, trade fairs, etc. relating to promoting cannabis and products derived from it. Any failure to respect this principle that there should be no promotion could lead to the immediate withdrawal of the permit and concession, and to claims for damages.
[1] European Monitoring Centre for Drugs and Drug Addiction (2019) Developments in the European cannabis market. EMCDDA Papers. Luxembourg: Publications Office of the European Union. Available at: http://www.emcdda.europa.eu/system/files/publications/11391/TDAU19001ENN.pdf
[2] Gates, P. J., Sabioni, P., Copeland, J., Le Foll, B., Gowing, L. (2016). Psychosocial interventions for cannabis use disorder. Cochrane Database of Systematic Reviews, 5 (CD005336). DOI: 10.1002/14651858.CD005336.pub4.
[3] Hoch, E., Preuss, U.W., Ferri, M., Simon, R. (2016). Digital Interventions for Problematic Cannabis Users in Non-Clinical Settings: Findings from a Systematic Review and Meta-Analysis. Eur. Addict. Res., 22:233-42.
[4] Tirado-Muñoz, J., Mestre-Pintó, J. I., Farré, M., Fonseca, F., Torrens, M. (2018) Comprehensive interventions for reducing cannabis use. Current Opinion in Psychiatry, 31(4):315–23. DOI: 10.1097/YCO.0000000000000430.
The existing monitoring and care system for potential problems linked to cannabis use should be expanded, with the following as its central elements:
- Monitoring of high-risk or potentially problematic use
- Evaluation of the form and intensity of use, accompanied by a diagnostic assessment
- Evaluation of the user’s needs, motivation and individual resources
- Proposal of tailored interventions and, where necessary, guidance towards specialist offerings
- Coordinated monitoring of patients following treatment
- Optimisation of access to consultation and help offerings, in particular by means of regionalising the extant offering
It seems essential to make customer-facing staff aware of the potential risks of cannabis use, of tools for monitoring and evaluating the form and severity of usage (e.g. approved questionnaires, such as the Cannabis Abuse Screening Test (CAST) and of existing care options. The involvement of general practitioners, emergency departments, schools and employers seems essential because they are often the first to encounter the various cognitive, mental or physical disorders, subsequently well documented, that could point to either use or misuse of cannabis.
In addition, particular attention should be paid to higher-risk groups (e.g. young people who are underperforming at school, facing troubled family situations or displaying signs of a mental disorder).
At the moment, no specific pharmacotherapies for cannabis-use disorders exist (Nielsen, 2019).[1] In the medium term, a full range of care offerings will have to be adopted at the national level, including out- and inpatient care for younger and older people, with and without prescribed medications, adapted in line with developments in the field; solution-focused brief therapy interventions for individuals, families and groups (see the Impuls service offered by Solina); online consultations; where necessary, residential rehabilitation stays at specialist facilities in- and outside Luxembourg; and follow-up care after treatment.
In addition to longer-term consultation and treatment options, the range of care offerings should include solution-focused brief therapy interventions for families, interventions based on cognitive behavioural therapy and motivational interviewing.
Good use will also have to be made of online consultations and of care for young people and their families.[2]
The above-mentioned interventions should be offered to beneficiaries according to their relevance, established on the basis of the individual monitoring and assessment stage. Lastly, patient follow-up should be ensured by means of sustained cooperation and coordination between the various specialists and non-specialists involved.
[1] Nielsen, S., Gowing, L., Sabioni, P., Le Foll, B. (2019) Pharmacotherapies for cannabis dependence. Cochrane Database of Systematic Reviews, 1 (CD008940). DOI: 10.1002/14651858.CD008940.pub3
Summary of the systematic literature review: The data are incomplete for all the pharmacotherapies examined and, on the basis of numerous evaluation criteria, the quality of the evidence was poor or very poor. The results show that SSRIs, SNRIs, bupropion, buspirone and atomoxetine are probably of little use for treating cannabis addiction. In view of the limited efficacy evidence, THC preparations must be considered to still be experimental, with some positive effects on withdrawal symptoms and syndrome. Little evidence is available on the anticonvulsant gabapentin, oxytocin and N-acetyl cysteine, but these medications merit further study.
[2] Examples: www.quit-the-shit.net, www.realize-it.org
PART III
PROSPECTS AND FUTURE DEVELOPMENTS
The working group takes the view that some aspects of the pilot project of access to cannabis for non-medical purposes should be re-evaluated at regular intervals. This will make it possible either to address challenges with practical implementation of the pilot project and of its goals, as set out in chapter I.3, or to take account of new data resulting from scientific evaluations or developments at the international level.
In that regard, it will be necessary to ensure that legislation and regulations are up to date in response to black-market and technological developments, not least because new ranges of cannabis preparation could emerge and methods of cannabis use could change.
It will be possible to introduce any changes that might be required into the national pilot project. It is therefore recommended to draw up a specific schedule, assessment criteria and an assessment process incorporated into the legislation.
Cannabis for non-medical purposes / non-medicinal cannabis
“Cannabis” means plants from the Cannabaceae family. The cannabis plant contains hundreds of chemicals, including more than 100 cannabinoids, along with flavonoids and aromatic terpenes. The effects of cannabis result from its cannabinoids acting on biological “targets”, a system of particular molecules and receptors found throughout the human body that, taken together, are called the endocannabinoid system. To date, two cannabinoids have been the subject of most of the scientific interest in the subject. Delta-9-tetrahydrocannabinol (THC) is the main psychoactive ingredient. When THC enters the bloodstream, it acts on the endocannabinoid receptors in the brain. THC acts in a dose-response relationship; high levels entering the bloodstream are more closely associated with negative health impacts. Cannabidiol (CBD) is the second cannabinoid that has been the subject of research. In Luxembourg, the cannabis available on the black market takes two main forms:
- flowering tops (dried)
- “hashish”, which is produced from cannabis plant resin
Regulation
Regulation is intended to enable, by means of the most appropriate policy and legal measures, individuals and society to limit the harm related to substance use; while there is no attempt to eradicate those substances, very restrictive measures are not ruled out, where applicable. It is, therefore, an approach intended to make a pragmatic contribution to controlling the relationship between people and drugs (or other types of product), with no argument being made for either the “war on drugs” or a putative future liberalisation.
Pilot project
A pilot project is a series of elements contributing to the achievement of a goal. It is scientific, temporary and limited in scope. A pilot project is intended to contribute to establishing evidence-based scientific foundations for decisions on potential later changes or future courses of action. The evidence obtained from a scientific assessment (see II.3) must be methodologically robust and lead to scientifically valid knowledge.
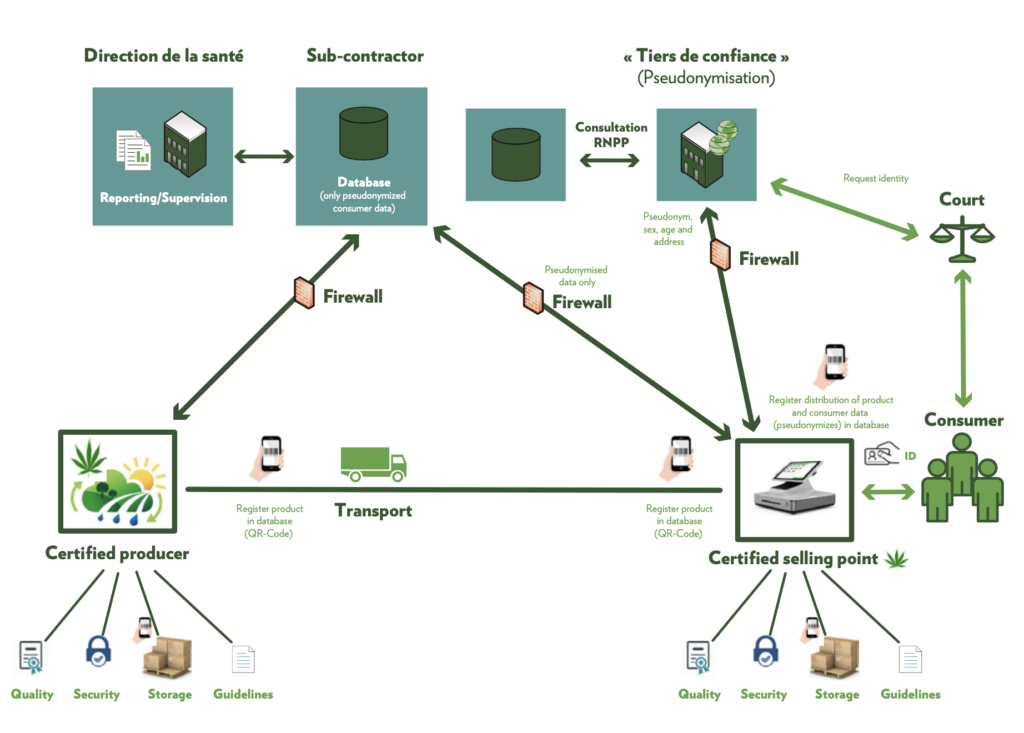
- Anderson, M., Hansen, B., Rees, D., Sabia, J. J. (2019). Association of Marijuana Laws with Teen Marijuana Use. JAMA Pediatr., 173(9):879-881. DOI:10.1001/jamapediatrics.2019.1720
- Berndt, N., Seixas, R., Origer, A. (2021). National Drug Report 2021 (RELIS report) – The Drug Phenomenon in the Grand-Duchy of Luxembourg: Trends and developments. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
- Berndt, N., Seixas, R. (2019). European Web Survey on Drugs: national implementation among a targeted sample of recreational drug users in Luxembourg 2018. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
- Cerdá, M., Wall, M., Feng, T., Keyes, K. M., Sarvet, A., Schulenberg, J., O’Malley, P. M., Pacula, R.L., et al. (2017). Association of state recreational marijuana laws with adolescent marijuana use. JAMA Pediatr., 171(2):142-9. DOI:10.1001/jamapediatrics.2016.3624
- European Commission (2019). European plant variety database. Available at: http://ec.europa.eu/food/plant/plant_propagation_material/plant_variety_catalogues_databases/search/public/index.cfm?event=SearchVariety&ctl_type=A&species_id=240&variety_name=&listed_in=0&show_current=on&show_deleted
- Council of the European Union (2003). Council Recommendation of 18 June 2003 (2003/488/EC) on the prevention and reduction of health-related harm associated with drug dependence, OJ 3.7.2003, L 165/31. Brussels: Official Journal of the European Union. Available at: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2003:165:0031:0033:EN:PDF
- European Monitoring Centre for Drugs and Drug Addiction (2022). European Drug Report 2022: Key Issues. Luxembourg: Publications Office of the European Union. Available at: https://www.emcdda.europa.eu/edr2022_en
- European Monitoring Centre for Drugs and Drug Addiction (2019). EU Drug Markets Report 2019.Luxembourg: Publications Office of the European Union. Available at: http://www.emcdda.europa.eu/system/files/publications/12078/20192630_TD0319332ENN_PDF.pdf
- European Monitoring Centre for Drugs and Drug Addiction (2019). Developments in the European cannabis market. EMCDDA Papers. Luxembourg: Publications Office of the European Union. Available at: http://www.emcdda.europa.eu/system/files/publications/11391/TDAU19001ENN.pdf
- European Health Interview Survey (2014, 2019). EHIS data processed by the Luxembourg National Focal Point of the EMCDDA. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
- EUR-Lex (2010). Judgment of the Court (Second Chamber) – Josemans, Case C-137/09 (2010). Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A62009CJ0137
- Gates, P. J., Sabioni, P., Copeland, J., Le Foll, B., Gowing, L. (2016). Psychosocial interventions for cannabis use disorder. Cochrane Database of Systematic Reviews, 5 (CD005336). DOI: 10.1002/14651858.CD005336.pub4.
- Heinz, A., van Duin, C., Kern, M. R., Catunda, C., Willems, H. (2019). Trends from 2006 – 2018 in Health Behaviour, Health Outcomes and Social Context of Adolescents in Luxembourg. HBSC Luxembourg Trends Report – Health Behaviour in School-Aged Children: World Health Organization collaborative cross-national study (HBSC). In press. Luxembourg, Esch-sur-Alzette: University of Luxembourg.
- Hoch, E., Preuss, U.W., Ferri, M., Simon, R. (2016). Digital Interventions for Problematic Cannabis Users in Non-Clinical Settings: Findings from a Systematic Review and Meta-Analysis. Addict. Res., 22:233-42.
- Luxembourg National Health Laboratory (2021). Données de pureté de substances psychoactives illicites 2021 traitées par le Point Focal Luxembourgeois de l’OEDT. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
- Ministry of State – Central Legislative Service (1973). Act of 19 February 1973 on the sale of medications and the combating of drug addiction. Publication: 03/03/1973. Luxembourg: Ministry of State – Central Legislative Service. Available at: http://data.legilux.public.lu/eli/etat/leg/loi/1973/02/19/n1/jo
- Ministry of Sustainable Development and Infrastructure (2016). Plan général du Highway Code, Article 12, paragraph four. Luxembourg: Ministry of Sustainable Development and Infrastructure. Available at: http://data.legilux.public.lu/file/eli-etat-leg-code-route-20161028-fr-pdf.pdf
- Ministry of State (2018). Coalition Agreement (2018-2023). Luxembourg: Ministry of State. Available at: https://gouvernement.lu/dam-assets/documents/actualites/2018/12-decembre/Accord-de-coalition-2018-2023.pdf
- Ministry of State – Central Legislative Service (2018). Act of 20 July 2018 amending Act of 2018 February 1973 on the sale of medications and the combating of drug addiction, as amended. Publication: 01/08/2018; Effective date: 05/08/2018. Luxembourg: Ministry of State – Central Legislative Service. Available at: http://data.legilux.public.lu/eli/etat/leg/loi/2018/07/20/a638/jo
- United Nations (1961). Single Convention on Narcotic Drugs of 1961. New York: United Nations. Available at: https://www.incb.org/documents/Narcotic-Drugs/1961-Convention/convention_1961_en.pdf
- Nielsen, S., Gowing, L., Sabioni, P., Le Foll, B. (2019) Pharmacotherapies for cannabis dependence. Cochrane Database of Systematic Reviews, 1 (CD008940). DOI: 10.1002/14651858.CD008940.pub3
- Nutt, D., King, L. A., Saulsbury, W., Blakemore, C. (2007). Development of a rational scale to assess the harm of drugs of potential misuse. The Lancet, 369(9566):1047-53. DOI: 10.1016/S0140-6736(07)60464-4.
- European Monitoring Centre for Drugs and Drug Addiction (2005). EMCDDA Thematic Papers Illicit Drug Use in the EU: Legislative Approaches. Lisbon: European Monitoring Centre for Drugs and Drug Addiction. Available at: http://www.emcdda.europa.eu/attachements.cfm/att_10080_EN_thematics01_en.pdf
- European Monitoring Centre for Drugs and Drug Addiction (2019). European Prevention Curriculum: a handbook for decision-makers, opinion-makers and policy-makers in science-based prevention of substance use. Luxembourg: Publications Office of the European Union. Available at: http://www.emcdda.europa.eu/system/files/publications/11733/20192546_TDMA19001ENN_PDF.pdf
- European Monitoring Centre for Drugs and Drug Addiction (2019). Drug profiles – cannabis. Available at: https://www.emcdda.europa.eu/publications/drug-profiles/cannabis_en
- Luxembourg Judicial Police Service – Drug Squad (2021). Données de pureté de substances psychoactives illicites 2021 traitées par le Point Focal Luxembourgeois de l’OEDT. Luxembourg: Luxembourg National Focal Point of the EMCDDA, Department of Epidemiology and Statistics at the Directorate of Health.
- Tirado-Muñoz, J., Mestre-Pintó, J. I., Farré, M., Fonseca, F., Torrens, M. (2018) Comprehensive interventions for reducing cannabis use. Current Opinion in Psychiatry, 31(4):315–23. DOI: 10.1097/YCO.0000000000000430.